
PODIUM. Journal of Science and Technology in Physical Culture, May-August; 2022, 17(2): 758-779
Translated from the original in spanish
Original article
Education in health, prevention and management of back pain under the approach "integration school community from the area of Physical Education"
Educación en salud, prevención y manejo del dolor de espalda bajo el enfoque "integración escuela comunidad desde el área de Educación Física"
Educação sanitária, prevenção e gestão da dor lombar no âmbito da "abordagem integração escola-comunidade da área da Educação Física"
Efrén Mesías Palacios
Zumba1*![]() https://orcid.org/0000-0003-4413-3393
https://orcid.org/0000-0003-4413-3393
Richar Jacobo Posso Pacheco1![]() https://orcid.org/0000-0003-1279-9852
https://orcid.org/0000-0003-1279-9852
Laura Cristina Barba Miranda2![]() https://orcid.org/0000-0003-3325-3875
https://orcid.org/0000-0003-3325-3875
Bertha Susana Paz Viter3![]() https://orcid.org/0000-0001-9240-1941
https://orcid.org/0000-0001-9240-1941
1Central University of Ecuador. Ecuador.![]()
2Ministry of Education of Ecuador. Ecuador.![]()
3National University of Chimborazo. Ecuador.![]()
*Corresponding author: empalacios@uce.edu.ec
Received: 07/03/2022.
Approved: 08/03/2022.
ABSTRACT
The purpose of the study was to assess the scope of an action plan for health education, prevention and management of back pain, with the School Community Integration approach from the Physical Education Area in the empowerment of knowledge and its application in favor of a comprehensive health to members of an educational institution in the city of Quito; it had as a methodological approach the socio-critical paradigm, according to the participatory action research method. Representatives of children enrolled in said institution are included as study subjects. The study was carried out in three stages. 1- Participatory diagnosis, where back pain appears as a frequent condition. 2- Preventive program that integrates anatomical, biomechanical, postural hygiene and exercise knowledge. 3- Evaluation of knowledge and skills acquired. Clinical history and determination of risk factors, application of pre and post-test related to back care, posture and exercises were performed. Based on the scores obtained and the observation of acquired skills, it is determined that the action plan allowed the acquisition of cognitive, behavioral and procedural values in all participants. The Community School Integration approach from the Physical Education Area is considered as a viable program of execution by the Ecuadorian Ministry of Education. These elements contribute to the maintenance, promotion and prevention of health conditions of community members.
Keywords: Health Education; Prevention; Back pain; School Community Integration Approach; Physical education.
RESUMEN
El estudio tuvo como propósito valorar los alcances de un plan de acción de educación en salud, prevención y manejo del dolor de espalda, con el enfoque Integración Escuela Comunidad desde el Área de Educación Física en el empoderamiento de conocimientos y su aplicación en pro de una salud integral a los miembros de una institución educativa de la ciudad de Quito; tuvo como enfoque metodológico el paradigma sociocrítico, según el método de investigación acción participativa. Se incluyen como sujetos de estudio a representantes de niños inscritos en dicha institución. El estudio se realizó en tres etapas. 1- Diagnóstico participativo, donde el dolor de espalda aparece como afección frecuente. 2- Programa preventivo que integra conocimientos anatómicos, biomecánicos, higiene postural y ejercicios. 3- Evaluación de conocimientos y habilidades adquiridas. Se realizó historia clínica y determinación de factores de riesgo, aplicación de pre y post- test relacionados con cuidado de espalda, postura y ejercicios. Se plantea sobre la base de puntajes obtenidos y observación de habilidades adquiridas se determina, que el plan de acción permitió la adquisición de valores cognitivos, conductuales y procedimentales en todos los participantes. Se considera el enfoque Integración Escuela Comunidad desde el Área de Educación Física como un programa viable de ejecución por parte del Ministerio Ecuatoriano de Educación. Estos elementos tributan al mantenimiento, promoción y prevención en condiciones de salud de los miembros comunitarios.
Palabras clave: Educación en Salud; Prevención; Dolor de Espalda; Enfoque Integración Escuela Comunidad; Educación Física.
RESUMO
O objectivo do estudo era avaliar o âmbito de um plano de ação para a educação sanitária, prevenção e gestão das dores lombares, utilizando a " Integração Escola - Comunidade da área da Educação Física" na capacitação do conhecimento e sua aplicação em favor da saúde integral dos membros de uma instituição de ensino na cidade de Quito; a abordagem metodológica foi o paradigma sócio crítico, de acordo com o método de investigação de ação participativa. Os representantes das crianças inscritas na instituição são incluídos como sujeitos de estudo. O estudo foi levado a cabo em três fases. 1- Diagnóstico participativo, onde a dor nas costas aparece como uma aflição frequente. 2- Programa preventivo integrando conhecimentos anatómicos e biomecânicos, higiene postural e exercícios. 3- Avaliação dos conhecimentos e das competências adquiridas. Foi realizado um historial clínico e determinação dos fatores de risco, aplicação de pré e pós-testes relacionados com cuidados de costas, postura e exercícios. Com base nas pontuações obtidas e na observação das competências adquiridas, foi determinado que o plano de ação permitiu a aquisição de valores cognitivos, comportamentais e processuais em todos os participantes. A abordagem Escola - Integração Comunitária da Área da Educação Física é considerada um programa viável para implementação pelo Ministério da Educação do Equador. Estes elementos contribuem para a manutenção, promoção e prevenção das condições de saúde dos membros da comunidade.
Palavras-chave: Educação para a Saúde; Prevenção; Dores de Costas; Abordagem Escola de Integração-Comunidade; Educação Física.
INTRODUCTION
Back pain has become a global health problem, and overuse and mechanical overload causing pain are the main causes of misuse of the spine due to improper posture; this exerts and causes a partial failure. This condition has enormous physical, psychological, social and economic consequences (Posso et al., 2022), which could be the result of the absence of learning and prevention programs for spinal care (Chavarria, 2014; Posso et al., 2022;). Improper use of the spine (movement and load handling position) causes back pain due to tension and discomfort in the musculoskeletal system. In the disorder, a number of conditions are derived including nerves, tendons, muscular structure support, intervertebral disc, etc.
These situations represent a wide range of illnesses that can range in severity from mild periodic symptoms to debilitating chronic conditions that can cause back pain. This symptom is associated with risk factors in three specific situations: a) activity at home b) work activity and c) state of the subject. Back pain, being one of the three most common causes of occupational disability, organizations and experts in charge of managing public health services have already expressed their concern about this health problem; They state that further research is needed on this topic Rivas, 2010).
Obesity stands out as a risk factor in the subject's own situation (Posso, 2018a). Significant abdominal expression causes an increase in intra-abdominal pressure, and displacement of the center of gravity counteracts lumbar lordosis. The process persistently increases the curvature and causes pain. Likewise, Reyes (2010) refers that tobacco and alcohol are vascular vasoconstrictors that reduce blood flow and oxygenation of the musculoskeletal structures and intervertebral disc. Here progressive degeneration occurs, and therefore, pain. For Gómez (2005), low back pain is also associated as a risk factor with "an intricate psychological cover for job dissatisfaction, boredom and a generous compensation system that contributes to it" (p. 2). There are also emotional and social factors that can influence the persistence of back pain. Likewise, it is considered that "the current clinical trend is oriented, in addition to the application of treatment, to prevention and patient education (p. 6).
The prevention of low back pain is based on the action of three fundamental pillars: avoiding weight loads inappropriately, postural hygiene and performing exercises (Chavarría, 2014). In Ecuador, there are public institutions with programs under an educational-preventive approach (Posso, 2018b). Educational institutions have been involved here; satisfactory results are obtained in its application as a therapeutic tool. Due to these effects, the integration approach has been incorporated into these programs (Posso et al., 2020), the community school from physical education; this incorporates the education of the individual to help them know their problem, manage it and avoid it. The integration of schools and communities from this approach, especially parents, implies a process of mutual participation in which each party and each member can contribute and receive what is in a defined account for the benefit of all. According to Pérez (2013), the integration of the community requires a series of agreements between the institution and the community to collaborate in planning; also contributes to the implementation and evaluation of programs or projects developed in the school and in the community (Posso et al., 2020).
In this order, Gómez (2019) points out that:
"School-Community integration is viewed as a systematic interweaving of interrelationships where individuals play to perform social and representative functions. They must voluntarily submit to a process of reciprocal understanding to coordinate the actions of their different members (parents, representatives, students, professors, teachers, neighbors)" (p.26).
In support of these initiatives of integration with the community, the Constitution of the Republic of Ecuador (2008), in its articles 26 and 343 on Education as Human Rights and Social Obligations, generally establishes that it is a public service oriented to the full development of creativity and personality (Posso et al., 2020). On the basis of respect for all currents of thought demonstrated by family values, the values of national and universal identity, they are recognized as a subject of education. This has been assumed by the majority of the world population (Posso et al., 2021) and at the center of the educational process. Meanwhile, the national educational system foresees the integration of intercultural visions according to the geographical, cultural and linguistic diversity of the country; also for respect for the rights of communities, individuals and nationalities.
The aforementioned raises the concern of applying an action plan for the prevention and management of back pain, which is based on the following premises:
That is why the group of authors of this research proposes as an objective: to assess the scope of an action plan for health education, prevention and management of back pain, with the School Community Integration approach from the Physical Education Area in the empowerment of knowledge and its application in favor of a comprehensive health to the members of an educational institution in the city of Quito.
To develop this study, they started from sources that allowed them to consult and transfer tools, methods and procedures that facilitated the work (Goetz and Le Comte 1988; Valles, 1997; Bru, 2003; Dick, 2005; Galeano, 2006; Rusque, 2008; Martínez, 2013).
MATERIALS AND METHODS
Design
This study is part of the educational policies of the Ministry of Education of Ecuador to meet the socio-community needs in the parameters of the specialty of each of its teachers. In this sense, the research is located within the socio-critical paradigm, and its design is based on participatory action research, to generate proposals in the field of health, in this area. Here it is considered that action research becomes a tool and support for the educational program and task, where two processes are combined; that of knowing and that of acting, involving in both the community which reality is addressed. In relation to the above, it is assumed that action research seeks to end the distance between those who decide and those who execute, between the researcher and the researched. It is about the conviction that participation will generate adherence to the course of action necessary for change. Action research is critically reflexive, that is, researchers and clients who, in turn, are co-researchers, regulate and systematically critically analyze what they are doing.
Participants
These participants represent the units of analysis; it is stated that these units made up of people are the ones that provide data and events to study. Attending to the guidelines by the authors and establishing as inclusion criteria that they were representatives of the community, including housewives, community leaders, among others. It was estimated that the participants were 10 after the group discussion and the focused interview, where they expressed their desire and commitment to participate in the research.
Procedure
With the collaboration and participation of the community doctor, as well as an intern in the rehabilitation area, a participatory diagnosis was made to identify the situations described above regarding back pain. In this way, a program could be established that leads to the education and prevention of this symptomatology; for this purpose, meetings were called in order to carry out the interview to guarantee the maximum possible participation. This gave rise to the expression and perspectives of the representatives of the community on which it is going to act. Community leaders, grassroots groups and organizations also originate. This allowed enriching the process, which results not only in the effectiveness of the diagnosis but also in the greater commitment of each and every one of the actors.
The diagnosis was carried out according to three moments: a) Initial interview; b) Introductory talk, registration and questionnaire application and c) Preparation of clinical history that includes: clinical and functional evaluation and determination of risk factors. The indicated evaluations allowed diagnosing the current state of health and showing the presence and degree of risk factors for spinal injuries present in each of the participants. Likewise, general laboratory tests and imaging studies of the spine previously performed when they went to medical consultations for back pain are reviewed.
On the other hand, workshops and education were held on commitment and participation in all stages of prevention and management of low back pain. It was proceeded through health education and health education, with a commonly used term in patient education, to better understand and manage the disease, achieve and maintain a better quality of life. In this way, a physical, mental, emotional and spiritual well-being is guaranteed, as a biopsychosocial being; Thus, the requirements set by the WHO regarding the prevention, maintenance and preservation of comprehensive health are met:
Data collection techniques and instruments
Participant observation
According to participant observation, it is the main qualitative data collection technique, since the researcher spent as much time as possible with the study participants, took part in their existence and reflected their interpretations and based on these, was able to induce interpretive comments based on their perceptions. In this sense, this type of information served to obtain from individuals their definitions of reality and the constructs that organize their world.
Measurement: this is based on a process capable of linking abstract concepts with empirical indicators, through an explicit and organized plan to be able to classify the available data, based on the concept that the researcher has in mind. The measurement consisted of clinical data from each of the participants to establish their health condition in a personalized way in terms of: blood pressure, heart rate, respiratory rate, body weight, height, abdominal circumference, determination of body mass index. Physical measurements were made at the beginning of the educational intervention process to determine the range of joint movements, muscle strength, flexibility, gait, posture, orthopedic alterations of the spine and lower limbs with the appropriate instruments and the necessary calculations to obtain the data.
Registry
The permanent and systematic recording of information is an essential condition to achieve the proposed objectives. The techniques by which the data referring to the continuous process in this research are collected refer to the learning of the biomechanical knowledge of the spine, risk factors and therapeutic tools. For this, the following was used: The focused interview, which was carried out when the group of participants was structured. The focused interview consists of a qualitative interview style aimed at paying attention to the cognitive and emotional sources of the interviewees. These act as subjects whose responses to the event are material for the study, rather than as informants of minimal events.
At the end of the interview, the questionnaire was applied as an instrument to establish the prior knowledge of each of the participants. They are related to: Back care, Weight Loads, Postural Habits and Practice of Physical Exercises. Here they also express motivation to participate and expectation of results at the end of the prevention program. Likewise, the group discussion was constituted as one of the main techniques of this research; this seeks to show a situation, which leads to reflect on its conditions, possibilities and consequences in order to improve or change them.
It is stated that, in this study, the participants of a discussion group express their experiences and provide information without modifying that of the others; it is not an attempt to impose oneself, but rather to contribute ideas. Based on what was described, the discussion group technique proposed by Participatory Action Research was used from its initial phase, when informal interviews were conducted to detect the health situation frequently presented by the inhabitants of the XXXXXXXXXX community. For this, a video recorder was used, a notebook to record identification data of the participating population. Their telephone numbers are included in this work to coordinate future discussions and also to point out details of interest to the study.
The interpretation of the information is a combined position between the researcher's position and the subjects' own interpretation regarding the responsibility to assume the necessary changes for their spinal health. Coding and categorization techniques were used, personally for each version, under the model proposed by the collaborating physician. The participatory diagnosis allowed a dialogue with each one of them and the obtaining of initial data for the elaboration of the educational program. A generalized structure is created in each work session, in turn the process of action research reaffirms the cycle that supports the transformation of the social reality of these subjects within the action-reflection-action cycle.
This cycle was visualized in the daily and professional postures and actions of each one of them, the conceptualization of the problem that is represented in the health of the spinal axis led the versionants to reflect on the postures and activities executed in an inadequate way to return to conceive an action in the correction, maintenance and prevention of vertebral health. It should be noted that a combination of quantitative techniques (descriptive statistics) was also applied.
RESULTS
Participatory diagnosis
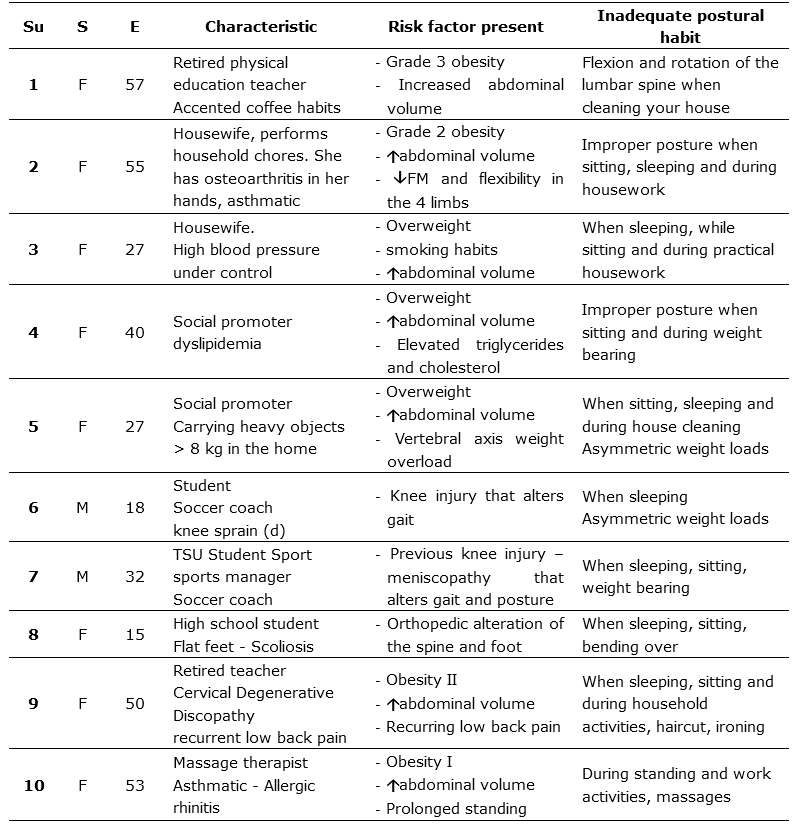
Table 1 shows what was expressed by subjects, in relation to the need to know the cause of their back pain and how to manage it to avoid it, improve it and even eliminate any cause that generates said pain. All the participating subjects stated that they had experienced back pain at some time and during the development of the program, 7 out of 10 subjects reported presenting back pain at the time.
This situation motivated the participants to develop and self -apply the prevention guidelines to obtain the health of their back. Additionally, a multiplier process was generated by extending their new theoretical and practical knowledge to the rest of their relatives. With this beginning, action research was evidenced in the back health program to solve their health problems related to this aspect, including improving their performance in their daily and work activities (Table 1).
Table 1. - Interpretation of the data extracted from the registration form
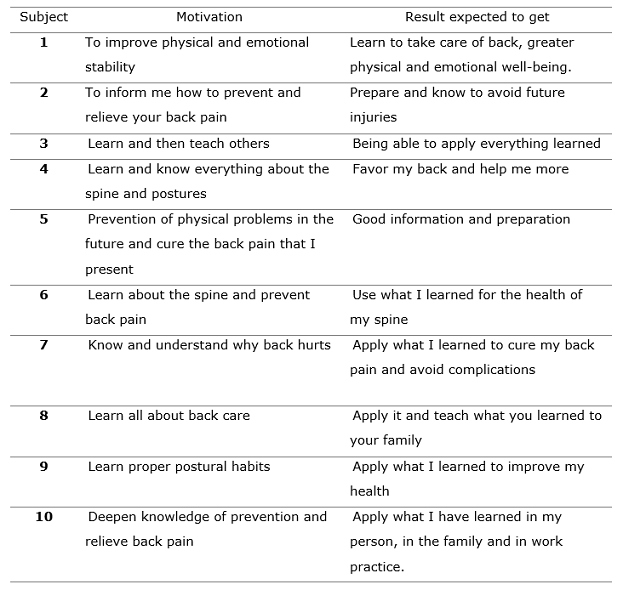
Table 2 shows the data of the functional evaluation and the measurement of basic clinical indicators. This allowed characterizing each subject against the ranges of normality indicated from the various universal patterns. In addition, the self-knowledge of these allowed a start of reflection among the subjects, which may represent risk factors for the health of their back. Next, graphs 1, 2, 3. 4. 5. 6, 7 and 8 show the graphs that make it possible to explain the clinical measurements obtained (Table 2) and (Figure 1).
Table 2. - Functional assessment and measurement of basic clinical indicators
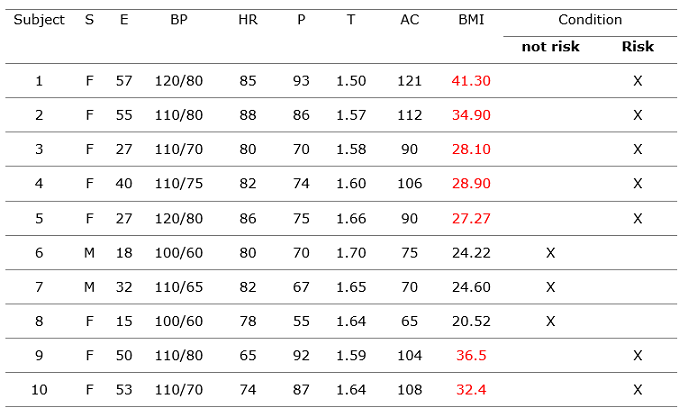
Legend: S = Sex; E = Age; BP = Blood Pressure (12/8). HR= Heart rate (60-80) P= Weight in Kg T: Height (mts ). AC: Abdominal circumference (Women < 80; men < 90). BMI: Body Mass Index: Normal (18 - 24.9); Overweight (25 - 29.9); obesity I (30 - 34.9); obesity II (35 - 39.9); obesity III (40 - 44.9); morbid obesity (45 - 49.9).
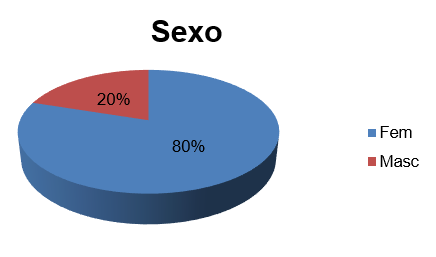
Fig 1 . - Percentage of participants according to gender
The representation of the participating sample was made up of 80% female and 20% male. The significance is considered that even when back pain is not established a prevalence according to sex, women are the first to attend to an alarm situation in their health. They are also the ones who are most exposed when combining occupational exposure with household activities, child care and the very fact of motherhood that increases the degree of curvature of the lumbar lordosis (Figure 2).
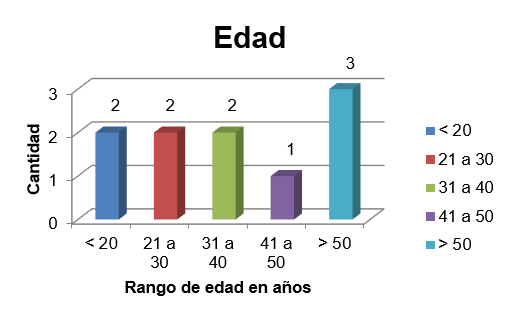
Fig 2. - Distribution of participants according to age
The age of the participants was between 18 and 58 years old, their manifestation was having suffered back pain at some time in their life . Here it becomes relevant that pain is not subject to age, but to other causes and/or risk factors, so that a first injury or transitory damage occurs. Crossing this data with work activities, inadequate postural habits and carrying out activities in a dysergonomic way implies a strengthening of the factors that have an impact on the occurrence of back pain (Figure 3).
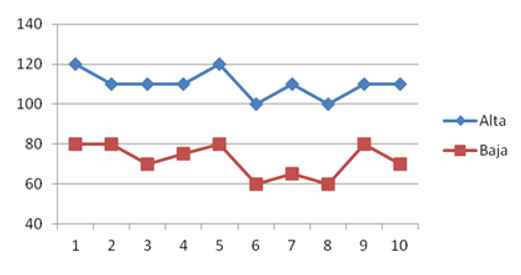
Fig 3. - Blood pressure values for each participant
In the blood pressure indicator, it was observed that all the participants were within the normal ranges, even when there were controlled hypertensive subjects. In this case, an altered blood pressure can generate anxious states, anguish and fear for thinking that it will give them a Cerebrovascular Accident (CVA) (Figure 4).
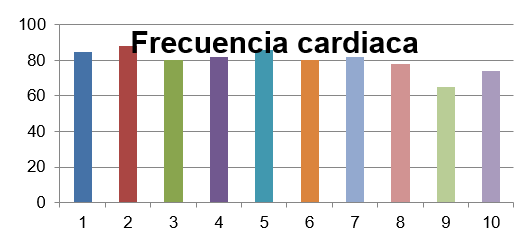
Fig. 4. - Heart rate values for each participant
The heart rate observed during the evaluations remained between 78 and 88 bpm , which was recorded in the initial clinical history in basal conditions of previous rest. The normal value ranges for an adult are between 60 and 100 bpm , for which the group studied remained within these limits. Heart rates could rise in situations of stress, anxiety, anguish, overweight, obesity and in the presence of back pain (Figure 5).
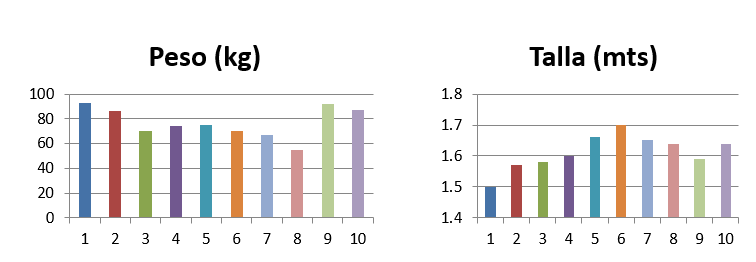
Fig 5. - Weight and height values for each participant
In relation to the weight and height indicators, an inverse relationship was observed between both variables. That is, the participants of smaller size have the highest body weight, this condition implies an inadequate mechanical load for the axial axis of the vertebra; it becomes an important factor for the appearance of back pain and consequently damage to the vertebral axial axis (Figure 6).
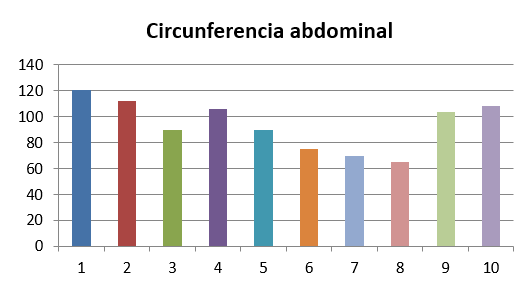
Fig 6. - Values of abdominal circumference for each participant
The range of abdominal circumference established as normal differs according to sex, the maximum limit for women should be less than 80 cm and for men less than 90 cm. In the measurements carried out, it was found that two male participants have an abdominal circumference in the normal range, of the eight female participants, only one meets the range. In other words, seven of the ten research subjects have a prominent abdomen, which produces an increase in intra-abdominal pressure, displacement of the axis of gravity towards the posterior area, which generates an increase in physiological lumbar lordosis and mechanical overload, be these factors of occurrence of back pain (Figure 7).
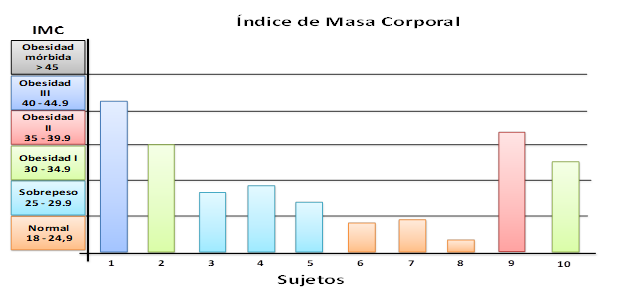
Fig. 7. - Body mass index values for each participant
Of the ten research subjects, seven are outside the normal range established for the Measurement of Body Mass Index. In other words, the result of applying the established formula is greater than 24.9 in 70 % of the cases, distributed as follows: one has type III obesity, two have type I obesity and 4 have overweight. Being overweight and obese are factors that considerably increase the risk of suffering from back pain; they cause mechanical overload of the vertebral axis, produce pain and tension at the muscular level and pain and damage to the joints due to the additional effort made by the muscles to support and move the body (Figure 8).
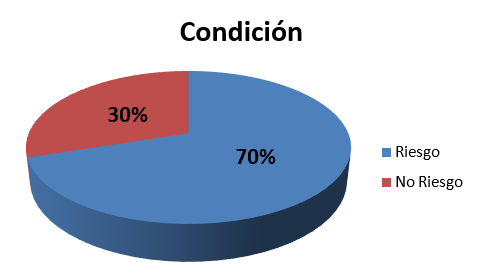
Fig 8. - Percentage distribution of the participants according to their condition
The measurements of the clinical parameters provided the initial information for each subject about the risk factors intrinsic to their physiological condition. This personal characterization is the first knowledge of the participants to take responsibility for the health status of their back; these factors cannot be determined in isolation, but in the integration that as a biopsychosocial being. In this case, they must attend to all the elements that they themselves can control, minimize, eliminate and unlearn old and harmful habits for the development of adequate health habits that imply a global well-being of health. They must behave in order to be successful and improve their standard of living. The result of the measurement carried out allows diagnosing that the health situation of the participants reflected 70% of subjects with anatomical and biomechanical risks that affect the appearance of back pain. Below, in Table 3, an interpretation is presented by conditions for each participant, which served as the basis for decision-making on their own health status and for the preparation of the action plan to be implemented.
Table 3. - Characterization of the participants according to risk factors and postural habits
Findings after the execution of the action plan
To establish the order in the interpretation of the information, it begins with the correspondence of the proposed purposes, in this case being carried out through the application of instrument 1 and 2, and the respective evaluation in relation to back care, postural hygiene and exercises.
The figures allow establishing the level of knowledge possessed by the participants (Figure 9) and (Figure 10).
Fig. 9 - Percentage distribution of the participants and comparison of the initial and final evaluations of knowledge about back care
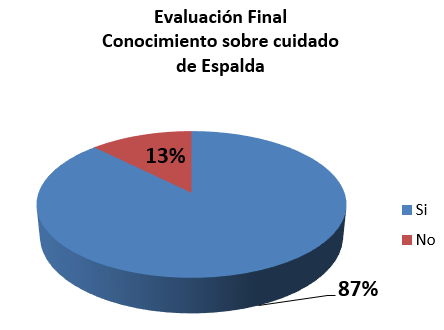
Fig. 10. - Percentage distribution of the participants and comparison of the initial and final evaluations of knowledge about back care
About back care, specifically related to its actions to apply care, figure 9 shows the results of the initial evaluation; it is observed in fuchsia color representing 40% the degree of ignorance, and in blue color with 60% the degree of knowledge present in the participants. By establishing the comparison between the results of the initial and the final evaluation, it is determined how there was an increase in the acquisition of knowledge; this is located at 87 %. This evidences a maintenance routine of ingrained habits that deserve greater support from the educational and communicational point of view to give way to an elimination of existing inappropriate habits and consequently adapt all participants to the acquisition of back care habits. of permanent application in all the activities of their daily life (Figure 11) and (Figure 12).
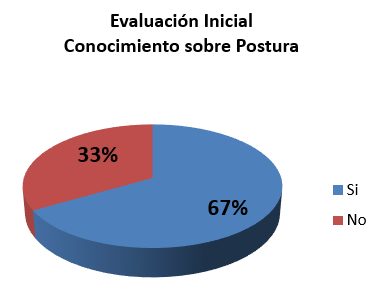
Fig. 11. - Percentage distribution of the participants and comparison of the initial and final evaluations of posture knowledge
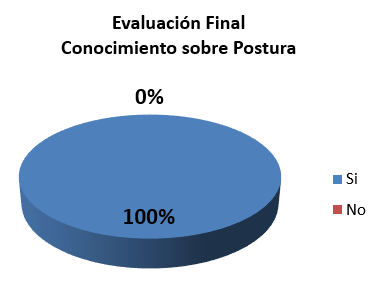
Fig. 12. - Percentage distribution of the participants and comparison of the initial and final evaluations of posture knowledge
When interpreting the information in relation to postural habits, the results of the initial evaluation can be seen in figure 11. It is perceived that 37 % of the participants do not know the proper postural habits to avoid back pain, in opportunely motivating contrast is that 67 % do know and execute adequate postural habits. When establishing the comparison between the results obtained in the final evaluation, it was very favorable to show that 100 % of the participants learned and applied all the postural rules correctly when carrying out the activities of daily life and work (Figure 13 and (Figure 14 ).
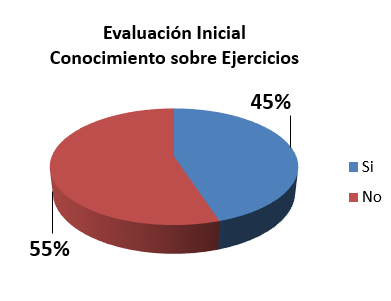
Fig. - 13. - Percentage distribution of the participants and comparison of the initial and final evaluations of posture knowledge
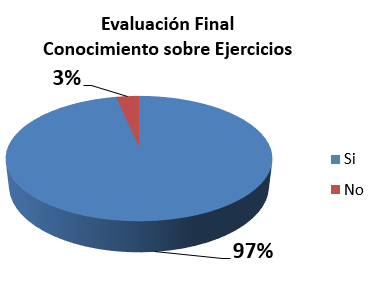
Fig. - 14. - Percentage distribution of the participants and comparison of the initial and final evaluations of posture knowledge
In relation to the knowledge about whether the practice of exercises prevents and helps to manage back pain, in the initial evaluation, 55 % of ignorance is registered in this regard against 45 % of adequate knowledge. After completing the action plan and performing the final evaluation, it is established that there was a comparatively significant increase in the knowledge and practice of physical exercises. It is evident in figure 13, that 97 % of the participants were trained in the practice and correct execution of exercises that will have an impact on the prevention, maintenance and conservation of the health of their back and body in general. It is known that the routine practice of physical exercises produces benefits to all the systems of the organism; the participant is made to feel happier, more energetic and with a desire to live, which in turn stimulates his immune system and protects him from the appearance of other pathologies.
DISCUSSION
The health education action plan executed to promote the school-community integration approach from Physical Education, met the particular conditions of the participants and allowed the acquisition of cognitive, procedural and behavioral values in all the participants. Thus, there is evidence of an increase in all the lines evaluated in the initial evaluation contrast of knowledge related to back care, postural habits and exercise practice and its final evaluation. Maintenance and prevention in the health conditions of community members are promoted. In this regard, Rull, Miralles and Mirralles (2010) consider that risk factors predispose the existence of biomechanical and anatomical alterations that compromise the health of the back. For his part, Dugdale (2011) states that emotional states such as anxiety contribute to and worsen back pain.
The study made it possible to assess the effectiveness of the action plan from the aforementioned approach through physical education, which provides practical theoretical elements on postural hygiene and back pain management, as based on Lorenzo and García (2009). They affirm that these processes reveal the absence of habits and knowledge about postural education. This allows understanding and improving attitudes regarding back care. Likewise, Alvarado de Parra (2000) affirms that every educational program serves as a model in the promotion of healthy behaviors; This effectively prevents the appearance of back pain that affects a large part of the population.
Establishing the level of knowledge that community members have about back care allowed planning the guidelines of the action plan to be executed. On the other hand, the participants were made aware of the existence of prevention programs called back school; it is shown that they are a health education program under the school-community integration approach from physical education. It is emphasized that they are terms that are completely unknown to them. In contrast, these fit perfectly to be applied and achieve the primary function, perform prevention and management of back pain. This agrees with the vision of Escalona (2010), which establishes that people should know or have information about the normal degenerative process caused by age, this accentuates the possibility of presenting back pain.
In the same order of ideas, Rojas (2008) states that the objective of postural hygiene is to learn to carry out the efforts of daily life in the most appropriate way possible; This decreases the risk of back problems. Although for those who already suffer from spinal pain, if they know how to make daily efforts they can improve their autonomy. This improves your daily activity, as it is not limited or the impact on it is minimal. For his part, Reyes (2010) notes that the prevalence of musculoskeletal conditions can be modified through an educational program in postural hygiene, and that this can be applied to healthy people, to prevent the risk of injury and to sick people; this reduces its limitation and improves its autonomy. In another particular, the study provided information on the prevention of back pain, which agrees with Vidal, (2020).
CONCLUSIONS
This concluded that health promotion in schools is possible through the application of intervention strategies based on postural education.
REFERENCES
Alvarado de Parra, K. (2000). Aplicación y evaluación de un programa educativo en la prevención del dolor de espalda en el personal de enfermería que labora en el ambulatorio urbano tipo III "Dr. Daniel Camejo Acosta" Barquisimeto estado Lara. http://bibmed.ucla.edu.ve/DB/bmucla/edocs/textocompleto/TWE720A582000.pdf
Bru, P. (2003). La investigación-Acción Participativa como metodología de mediación e integración sociocomunitaria. http://www.pacap.net/es/publicaciones/pdf/comunidad/6/documentos_investigacion.pdf
Chavarría, J. (2014). Lumbalgia. Causas, diagnóstico y manejo. Rev Médica de Costa Rica y Centroamérica. LXXI (611):447-54. http://www.medigraphic.com/pdfs/revmedcoscen/rmc-2014/rmc143n.pdf
Constitución, (2008). Constitución de la República del Ecuador. Quito: Medios públicos E.P.
Delgado, J. (1994). Métodos y Técnicas Cualitativas de Investigación en Ciencias Sociales. Editores: Síntesis.ISBN: 84-7738-226-3. https://dialnet.unirioja.es/servlet/libro?codigo=491811
Dick, B. (2005). Investigación Acción: Estrategias Cualitativas de la Investigación. Caracas Venezuela: Candidus Editores Educativos.
Dugdale, D. (2011). El dolor y sus emociones. Medline Plus. http://www.nlm.nih.gov/medlineplus/spanish/ency/patientinstructions/000417.htm
Escalona, E. (2010). Ergonomía en centros sanitarios y Prevención de lesiones musculoesqueleticas. http://www.bvs.org.ve/jornadas2010/01122010/Foros/EscalonaEvelyn.pdf
Galeano, M. (2006). Diseños de proyectos en la Investigación Cualitativa. Universidad Eafit, 2020. ISBN: 9789588173788http://books.google.co.ve/books?id=ufsZQkjMUFEC&printsec=frontcover&hl=es&source=gbs_ge_summary_r&cad=0#v=onepage&q&f=false
Goetz, J.P. y Le Compte, M.D. (1988). Etnografía y diseño cualitativo en investigación educativa. Madrid, España: Morata. Caps. IV y V. https://books.google.com.cu/books/about/Etnograf%C3%ADa_y_dise%C3%B1o_cualitativo_en_inv.html?id=rXESvgAACAAJ&redir_esc=y
Gómez, L. (2005). Lumbalgia o dolor de espalda baja. Artículo publicado en Revista Mexicana de Algología. http://www.intramed.net/sitios/mexico/dolor/VOLV_2_1.pdf
Gómez, L. (2019). Comunicación e Información en el ámbito educativo. México. Editorial Trillas.
Gómez, M. (2006). Introducción a la Metodología de Investigación científica. http://www.intramed.net/sitios/mexico/dolor/VOLV_2_1.pdf
Lorenzo, M y Garcia J (2009). Elaboración y aplicación de un programa de educación postural en educación secundaria. Facultad de Ciencias de la Educación. Pontevedra Universidad de Vigo. Disp. http://webs.uvigo.es/reined/ejemplares/2/reined_02_04.pdf
Martínez, M. (2013) La Investigación Cualitativa. (Síntesis conceptual), 1ra edición, México. Editorial Trillas. https://sisbib.unmsm.edu.pe/bvrevistas/investigacion_psicologia/v09_n1/pdf/a09v9n1.pdf
Posso, R. (2018a). Guía de estrategias metodológicas para Educación Física. Quito: Ministerio de Educación. https://educacion.gob.ec/wp-content/uploads/downloads/2019/01/GUIA-METODOLOGICA-EF.pdf
Posso Pacheco, R. J.., Barba Miranda, L. C., & Otáñez Enríquez, N. R. (2020). El conductismo en la formación de los estudiantes universitarios. Revista EDUCARE - UPEL-IPB - Segunda Nueva Etapa 2.0, 24(1), 117133. https://doi.org/10.46498/reduipb.v24i1.1229Vera
Posso Pacheco, R., Barba Miranda, L., Rodríguez-Torres, A., Núñez Sotomayor, L., Ávila Quinga, C. y Rendón Morales, P. (2020). An Active Microcurricular Learning Model: A Guide to Classroom Planning for Physical Education. Revista Electrónica Educare, 24(3), 294-311. https://dx.doi.org/10.15359/ree.24-3.14
Posso Pacheco, R., Barba Miranda, L., León Quinapallo, X., Ortiz Bravo, N., Manangón Pesantez, R. y Marcillo Ñacato, J. (2020). Educación Física significativa: propuesta para la contextualización de contenidos curriculares. Podium. Revista de Ciencia y Tecnología en la Cultura Física, 15(2), 371-381. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1996-24522020000200371&lng=es&tlng=es.
Posso Pacheco, R. J., Pereira Valdez, M. J., Paz Viteri, B. S. y Rosero Duque, M. F. (2021). Gestión educativa: factor clave en la implementación del currículo de educación física. Revista Venezolana De Gerencia, 26(Número Especial 5), 232-24. https://www.produccioncientificaluz.org/index.php/rvg/article/view/36442
Posso Pacheco, R. J., Ortiz Bravo, N. A., Paz Viteri, B. S., Marcillo Ñacato, J. y Arufe Giráldez, V. (2022). Análisis de la influencia de un programa estructurado de Educación Física sobre la coordinación motriz y autoestima en niños de 6 y 7 años. Journal of Sport and Health Research. 14(1). 123-134. https://recyt.fecyt.es/index.php/JSHR/article/view/86055/67703
Posso Pacheco, R. J. (2022). La post pandemia: una reflexión para la educación. MENTOR Revista De investigación Educativa Y Deportiva, 1(1), 1-6. https://revistamentor.ec/index.php/mentor/article/view/2118
Rivas, S. (2010). Manejo del síndrome doloroso lumbar. Rev Cubana Med Gen Integr. 26(1). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252010000100013
Rull, M., Miralles, R.C. y Mirralles, I. (2010). Dolor de espalda diagnostico enfoque general del tratamiento. Hospital Universitario de Tarragona. http://www.scartd.org/arxius/lumbalgia_rull05.pdf
Rusque, A. (2008). Enfoque Cualitativo. http://nulan.mdp.edu.ar/705/1/00369.pdf
Valles, M. (1997). Técnicas Cualitativas de Investigación. Madrid, España. Editorial Síntesis.
Vidal, J. B. (2020). Alteraciones hematológicas y COVID-19. Medicina balear, 35(4), 69-73. http://www.scielo.org.co/pdf/nova/v18nspe35/1794-2470-nova-18-spe35-75.pdf
Conflict of interests:
Los autores declaran no tener conflictos de intereses.
Authors' contribution:
The authors have participated in the writing of the work and analysis of the documents.
![]()
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0
International license
Copyright (c) 2022
Efrén Mesías Palacios Zumba, Richar Jacobo Posso Pacheco, Laura Cristina Barba Miranda, Bertha Susana Paz Viteri