
PODIUM. Journal of Science and Technology in Physical Culture, September-December 2022; 17(3):1174-1193
Translated from the original in spanish
Original artícle
Program of therapeutic physical activities for pregnant women with gestational diabetes
Programa de actividades físicas terapéuticas para embarazadas con diabetes gestacional
Programa de atividade física terapêutica para mulheres grávidas com diabetes gestacional
Nadia Haydeé Sánchez
Rosabal1*![]() https://orcid.org/0000-0002-8804-3595
https://orcid.org/0000-0002-8804-3595
José Ezequiel Garcés
Carracedo2![]() https://orcid.org/0000-0001-6340-9450
https://orcid.org/0000-0001-6340-9450
Lexy Lázaro Figueredo2![]() https://orcid.org/0000-0002-8753-8481
https://orcid.org/0000-0002-8753-8481
Alexis Macías Chávez2![]() https://orcid.org/0000-0003-4617-7728
https://orcid.org/0000-0003-4617-7728
1Raúl Podio Saborit Teaching Polyclinic. Rehabilitation room. MINSAP. Granma. Cuba.![]()
2Faculty of Physical Culture of the University of Granma. Cuba.![]()
*Corresponding author: sanchezrnadia@gmail.com
Received:2022-06-25
Approved:2022-10-08.
ABSTRACT
Introduction: The physical activity professional helps with important contributions to the
programs, applies health education and strengthens the physical and psychological preparation of
the population. Hence, the research was focused on showing the results of a program of
therapeutic physical activities.
Objective: The objective of this work was to develop a program of therapeutic physical
activities, characterized by a comprehensive approach in health education that allows a better
prescription in the biopsychosocial preparation of pregnant women with gestational diabetes in achieving
a satisfactory delivery.
Materials and methods: For this, a study of pre experimental of minimum control design
was carried out, with a duration of three years (2019-2021). The selected sample was made from
a stratified, non-probabilistic intentional sampling. Theoretical and empirical methods were used,
as well as research techniques, among which analysis and synthesis, inductive-deductive,
systemic-structural functional, documentary analysis, structured observation, interview and survey
stand out.
Results: The program was carried out through the implementation of therapeutic physical
exercises. Sixteen pregnant women with gestational diabetes participated, more than 56% showed
high levels of anxiety, depression and stress. The 88% showed low levels of physical fitness. The
100% managed to positively modify behavior towards healthy lifestyles with good metabolic control.
The 94% achieved good physical and psychosocial condition, they also decreased the dose of insulin.
Conclusions: The study showed that the prescription in the biopsychosocial preparation
aimed at achieving a satisfactory delivery in pregnant women with gestational diabetes was improved.
Keywords: Therapeutic physical activity; Gestational diabetes; Pregnancy.
RESUMEN
Introducción: El profesional de actividad física contribuye con aportes importantes en
los programas, aplica la educación sanitaria y fortalece la preparación física y psicológica en
la población. De ahí que la investigación estuvo centrada en mostrar los resultados de un
programa de actividades físicas terapéuticas.
Objetivo: El objetivo de este trabajo consistió en elaborar un programa de actividades
físicas terapéuticas, caracterizado por un enfoque integral en educación para la salud que permita
una mejor prescripción en la preparación biopsicosocial de las embarazadas con diabetes
gestacional en el logro de un parto satisfactorio.
Materiales y métodos: Para ello, se realizó un estudio de diseño preexperimental de
control mínimo, con tres años de duración (2019-2021). La muestra seleccionada se realizó a partir de
un muestreo intencional estratificado, no probabilístico. Se emplearon métodos de los niveles
teórico y empírico, así como técnicas de investigación entre los que destacan análisis y síntesis,
inductivo-deductivo, sistémico-estructural funcional, análisis documental, observación estructurada,
entrevista y encuesta respectivamente.
Resultados: El programa se realizó mediante implementación de ejercicios físicos
terapéuticos. Participaron 16 embarazadas con diabetes gestacional, más del 56 % mostró altos niveles
de ansiedad, depresión y estrés. El 88 % evidenció bajos niveles de condición física. El 100 %
logró modificar de forma positiva el comportamiento hacia estilos de vida saludables con buen
control metabólico. El 94 % alcanzó buena condición física y psicosocial, también disminuyeron la dosis
de insulina.
Conclusiones: El estudio mostró que se mejoró la prescripción en la preparación
biopsicosocial orientada al logro de un parto satisfactorio en embarazadas con diabetes gestacional.
Palabras clave: Actividad física terapéutica; Diabetes gestacional; Embarazo.
SÍNTESE
Introdução: O profissional de atividade física contribui com importantes contribuições em programas, aplica educação sanitária e fortalece a preparação física e psicológica da população. Assim, a pesquisa foi focada em mostrar os resultados de um programa de atividades físicas terapêuticas.
Objetivo: O objetivo deste trabalho foi elaborar um programa de atividades físicas terapêuticas, caracterizado por uma abordagem integral na educação sanitária que permite uma melhor prescrição na preparação biopsicossocial de gestantes com diabetes gestacional na realização de um parto satisfatório.
Materiais e métodos: Para este fim, foi realizado um estudo de controle mínimo pré-experimental de três anos (2019-2021). A amostra selecionada foi baseada em amostragem estratificada, não probabilística e propositada. Foram utilizados métodos teóricos e empíricos e técnicas de pesquisa, incluindo análise e síntese, indutivo-dedutiva, sistêmico-estrutural-funcional, análise documental, observação estruturada, entrevista e pesquisa, respectivamente.
Resultados: O programa foi realizado através da implementação de exercícios físicos terapêuticos. Dezesseis mulheres grávidas com diabetes gestacional participaram, mais de 56% mostraram altos níveis de ansiedade, depressão e estresse. Oitenta e oito por cento mostraram baixos níveis de aptidão física. 100% foram capazes de modificar positivamente o comportamento em direção a estilos de vida saudáveis com bom controle metabólico. 94 % conseguiram uma boa aptidão física e psicossocial, eles também diminuíram a dosagem de insulina.
Conclusões: O estudo mostrou uma melhor prescrição na preparação biopsicossocial com o objetivo de obter um parto bem sucedido em mulheres grávidas com diabetes gestacional.
Palavras-chave: Atividade física terapêutica; Diabetes gestacional; Gravidez.
INTRODUCTION
Currently, diabetes is one of the chronic metabolic diseases with the greatest social impact, its prevalence worldwide has increased in the last two decades, it affects more than 463 million inhabitants. In Cuba more than a million people suffer from it. It is characterized by high levels of sugar in the blood, its incidence increases annually, it occupies the eighth cause of death and has a prevalence of 66.9 per thousand inhabitants (Health Statistical Yearbook, 2021).
The high incidence of diabetes is recognized by many as a true epidemic of the 21st century, the result of poor lifestyles of the population; It requires that the health authorities focus their efforts on combating this disease and treating all the complications derived from it early (Statistical Health Yearbook, 2020).
Diabetes is one of the most prevalent diseases in the modern world, a consequence, also, of the increase in obesity, inappropriate diet and sedentary lifestyle, the latter explained, in part, by the abuse of technology and the facilities of modernity. It represents one of the great current health problems, which extends to the pregnant woman with obstetric repercussions and in the life of the woman who follows the pregnancy (Vigil -De Gracia and Olmedo, 2017); World Health Organization (WHO, 2020).
Gestational diabetes is defined as the alteration of carbohydrate metabolism, which is detected during pregnancy and represents an important risk factor for women and a health problem for the product. It affects 1 in 25 pregnancies in the world. It constitutes the fourth group in the current classification of diabetes. (Dominguez et al., 2016); in Cuba, 4 % of pregnant women are diabetic. National Diabetes Institute, (IND, 2017).
Based on the above considerations, it is necessary to seek solutions that guarantee changes in attitudes in these women, since the risk factors and the symptoms they show constitute the entrance of complications if they do not receive adequate care. That is why the topic presented responds to the WHO recommendations on prenatal care as a positive experience of pregnancy.
Physical activity for pregnant women at the international and national level has been directed towards an adequate control of training, in this regard the main contributions belong to Fernández et al. (2007); Davenport et al. (2018); Barakat et al. (2019); who apply the exercise prescription; contributions that limit care for pregnant women with diseases.
Despite the efforts made by these physical programs in order to improve the psychophysical preparation of pregnant women through the prescription of physical exercise, they do not take into account those who suffer from illnesses, they do not include the linked participation of all the health facilitators responsible for this task; They also do not have methodological and evaluative resources, important aspects in the benefit of childbirth.
Data offered by specialists from the Health Directorate and the Sports Directorate of the Media Luna Municipality in the province of Granma, indicate that, in the last ten years, there has been a notable increase in pregnant women processed for the health areas and the areas Therapeutic Physical Culture with a diagnosis of gestational diabetes, which demonstrates the need to carry out a physical activity program that allows the control and treatment of pregnant women who suffer from it.
Various researchers and organizations both internationally and nationally allocate their efforts to the treatment of gestational diabetes in the context of physical activity, the main references correspond to Fernández, (2016); the ADA, (2021) and American College of Obstetricians and Gynecologists, (ACOG , 2018); who approve the need for the practice of physical exercise in metabolic control. However, their conceptions lack theoretical-methodological foundations to establish their programming, prescription and adaptation for gestational diabetes.
The studies discussed above estimate an attempt to apply physical activities for the treatment of gestational diabetes; despite this, it is not perceived as a systemic and dosed care process that encompasses the biological and psychosocial aspects in all its dimensions, since there are still contradictions between the prescription of physical exercise, the prejudice of the benefits that its practice reports and the participation of health facilitators for a comprehensive work that allows adequate care.
The main intention of the work is to develop a program of therapeutic physical activities, characterized by a comprehensive approach in health education that allows a better prescription in the biopsychosocial preparation of pregnant women with gestational diabetes in the achievement of a satisfactory delivery.
MATERIALS AND METHODS
The study was carried out with a pre -experimental type design of minimal control; it is fulfilled through an initial and final test, in which after the first diagnosis the independent variable is handled, with the application of the program and later it is evaluated in the final verification and its effectiveness is verified.
The present research was developed in the therapeutic area of Physical Culture of the Media Luna municipality (Granma), with a duration of three years (2019-2021).
The selected sample was made from a stratified, non-probabilistic intentional sampling, pregnant women with gestational diabetes were taken into account as the unit of analysis. From a population of 23, 16 (69%) were selected, mean age 36 years.
Only four pregnant women are given insulin. For the development of the research, it was determined to include pregnant women, under the following inclusion and exclusion criteria:
Inclusion criteria: pregnant with gestational diabetes, being endorsed by the obstetrician-gynecologist to perform physical activity and not participating in another program.
Exclusion criteria: absolute medical contraindications: metabolic lack of control. Second Cuban Consensus on Diabetes and Pregnancy. Active cardiomyopathy, heart failure and rheumatic fever II, thrombophlebitis, recent pulmonary embolism, severe hypertension, acute infection, cervical incompetence, severe iso -immunization, multiple pregnancy, CIUR, fetal macrosomia, genital hemorrhage, premature rupture of ovular membranes, lack of control prenatal care, fetal distress, and risk of preterm birth.
Exit criterion: systematic attention is not reached.
Sixty-six health facilitators responsible for caring for pregnant women were incorporated.
Theoretical and empirical methods and research techniques were used, including: analysis and synthesis, inductive-deductive, systemic-structural functional, documentary analysis, methodological triangulation and by sources, structured observation, interview and survey.
Physical activities were observed (symptoms shown by pregnant women with gestational diabetes, participation and interest in physical activity, ways of acting in their health care, health education, educational methods used by teachers and prescription in biopsychosocial preparation A self-assessment questionnaire on diabetes and pregnancy issues was developed.
The clinical history of the pregnant women was explored to find out risk factors for gestational diabetes and sociodemographic characteristics. Physical activity programs for pregnant women and diabetics were reviewed. Interviews with health facilitators (teachers of Therapeutic Physical Culture, transdisciplinary health team and community entities).
The evaluation of the prescription was carried out through the methodology and evaluation at high levels (positive), medium level (uncommon negative) and low level (negative).
The biological dimension evaluated three indicators:
The psychosocial dimension evaluated two indicators:
To assess the effectiveness of the therapeutic physical activity program, the evaluation of childbirth was carried out. in pregnant women with gestational diabetes.
Indicators: breathing-relaxation management in childbirth (sufficient, little or none), types of childbirth: induced, premature, term, postmature, normal, laborious and surgical. Obstetric and metabolic complications: tearing of the perineum, large fetuses, babies with low birth weight and malformations, spontaneous abortions, increased amniotic fluid, placental abruption, postpartum bleeding, neonatal death, preeclampsia, hypertension, hyperbilirubinemia, and respiratory problems.
RESULTS AND DISCUSSION
After obtaining the information through observation of physical activities, the self- assessment questionnaire on diabetes and pregnancy, the exploration of medical records, sociodemographic characteristics, physical activity programs for pregnant women and diabetics , interviews with health facilitators (teachers of Therapeutic Physical Culture, transdisciplinary health team and community entities), results were obtained from the Therapeutic Physical Culture process for pregnant women with gestational diabetes:
The characterization of pregnant women through the dimensions, indicators and established parameters revealed the following results:
As shown in figure 1 in the evaluation of the biological dimension of pregnant women with gestational diabetes, the results of the gestational diabetes criterion indicator determined that, through fasting blood glucose, only four pregnant women were diagnosed with this disease. In the OGTT parameter, which diagnoses gestational diabetes, it was determined that all pregnant women were classified with this disease; because the glycemia values exceed the normal figures (Figure 1).
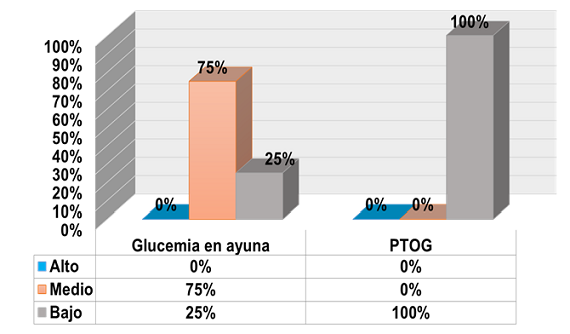
Fig. 1. - Results of the initial measurement applied to pregnant women in the indicator
criterion of gestational diabetes
Source: (SCCDE, 2018).
In the physiological control indicator, (Figure 2), the results derived from the BMI showed that pregnant women were overweight and moderately obese, which is a risk factor for gestational diabetes. These unfavorable results are due to the scarce pre-gestational exercise habits; since obesity according to the age of onset is post-pubertal as the size of the cell increases due to its high fat content. It is exogenous when receiving a supply of foods rich in calories and nutrients that is higher than energy expenditure due to problems with food consumption. Therefore, there are risks of other diseases.
The second parameter related to heart rate (HR) was altered, although there were no signs of bradycardia and tachycardia; this result according to Rigol and Santiesteban, (2014) may be related to the increase in HR 70-80 beat / min for hypertrophy of the heart to 12 %. Thus, its performance increases by 40 % and its peak in 20 to 24 weeks and >1.5 L/min of pregestational levels, depends on the effort that increases at the end of pregnancy and varies due to stress and exercise, the latter requires a correct planning and dosage that guarantees maternal-fetal health. Also due to compression of the uterus on the inferior vena cava, therefore decreases the return of venous blood to the heart.
In the parameter respiratory frequency (RF), it was evidenced that pregnant women revealed data of 26 respiratory movements per minute, a value slightly higher than normal and a pregnant woman showed increased values, when symptoms of fatigue and difficulties in expelling air were observed.
Hence the importance of preventing complications. It can also manifest as elevated because the uterus compresses the diaphragm and the vertical diameter of the thorax decreases, the vital capacity remains normal; chest circumference grows. The use of O2 and the basal metabolism increase, due to the sum of the feto-placental and maternal metabolism. The pregnant woman presents dyspnea without exertion related to psychological and cardiovascular factors.
Regarding systolic blood pressure (SBP), data were reflected that do not correspond to the normal parameters accepted during pregnancy, with decreased values and others increased. In this sense, the TAS declines little during pregnancy with small changes.
Related to the diastolic blood pressure (DBP), it can be reduced during pregnancy from week 12-26 and rises to its pre-gestational figures at week 36. In this way, slightly decreased values were shown. Therefore, the results show the inadequate habits and lifestyles of these pregnant women (Figure 2).
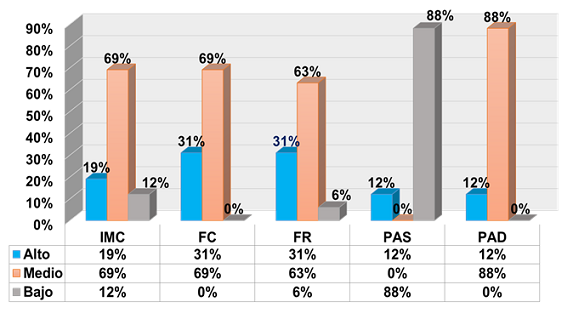
Fig. 2. - Results of the initial measurement applied to pregnant women in the physiological control indicator
Regarding the physical condition indicator, (Figure 3), the assessment of coordination skills for labor was carried out through demonstrations about how they simulated this coordination, which showed that pregnant women did not master the skill. The unfavorable results are due to the scarce habits of pre-gestational physical exercises that these pregnant women present.
Muscle strength parameter of the muscles involved in the birth canal; it was evidenced that pregnant women showed muscle weakness of the pelvic floor; this evaluation responds to the physical inactivity present in these pregnant women. Regarding the flexibility parameter of the pelvic floor, it was determined that the pregnant women were not able to reach an angle of 135 degrees from the position of lying back, arms down, bring their legs forward up, extended up to an angle of 135 degrees, they only reached 45 degrees.
The cardiorespiratory-metabolic endurance assessed by the 6-minute walk test adapted to these pregnant women allowed to know Vo2Máx, which determined that they showed symptoms of exhaustion and without momentum, they were classified in functional class III. This is due to physical inactivity and pregnancy that increase daily energy expenditure by meeting energy needs in additional basal metabolic rate and movement expenditure of greater body mass; hence the maternal-fetal organisms need to receive sufficient protein, fat, carbohydrates, mineral salts and vitamins.
In this regard, pregnant women at rest increase basal O2 consumption, due to greater cardiocirculatory, respiratory and renal activity, due to extra consumption by the fetus and the uterus and placenta; the use of glucose is reduced due to the decrease in sensitivity to insulin, the plasmatic value increases with a diabetogenic response, which does not favor the adequate supply of glucose to the fetus; in such a way that the lipolytic activity increases.
In the speech test that determines the effort made by pregnant women during physical exercise using the Borg scale, difficulties were found at the cardiorespiratory level, which is related to sedentary lifestyle, gestational diabetes and pregnancy that require greater energy expenditure. Regarding postural control, the results showed that pregnant women adopted inadequate postures, deformities mainly in the region of the feet, knees, back and spine, with symptoms of pain and discomfort.
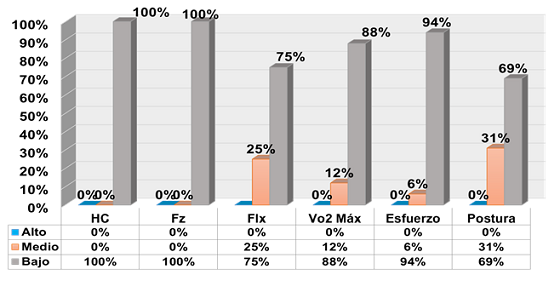
Fig. 3. - Results of the initial measurement applied to pregnant women in the physical condition indicator
In the evaluation of the psychosocial dimension, in the psychological well-being indicator, the state of anxiety showed that the pregnant women presented a high level of anxiety with opinions of little importance that jumped out of their imagination during physical activity, which intervened in their state of mind, they manifested melancholy; this is related to periods of stress, exhaustion quickly and little personal satisfaction.
The assessment of the results emanating from the state of depression, allowed to verify that the pregnant women showed concern, they imagined a desperate future that will not improve, with the desire to take their own life, to cry, insecurity and inability to do any job no matter how small, they tired easily, difficulty sleeping.
In vulnerability to stress, there was no extremely vulnerable pregnant woman; but they showed themselves to be seriously vulnerable, as they never exercised, their income did not meet their expenses, they did not attend social activities, they almost never made friends and they never had fun; however, they often slept well and were in good health (Figure 4).
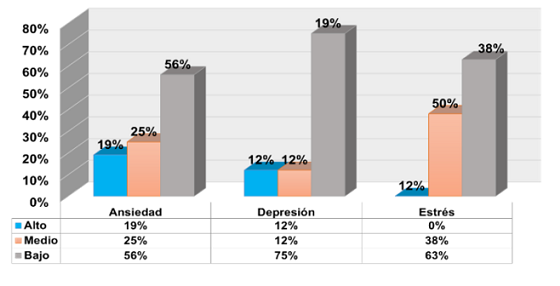
Fig. 4. - Results of the initial measurement applied to pregnant women in the indicator psychological well-being
The establishment of the social welfare indicator in interpersonal relationships and behavior towards the people with whom they interact, (Figure 5) pregnant women did not control their impulses before certain situations, they also did not show consideration and affection for people, they did not identify with the people they interact with and limited participation in activities. The unfavorable results respond to gestational diabetes and pregnancy, which demonstrates inappropriate ways of acting.
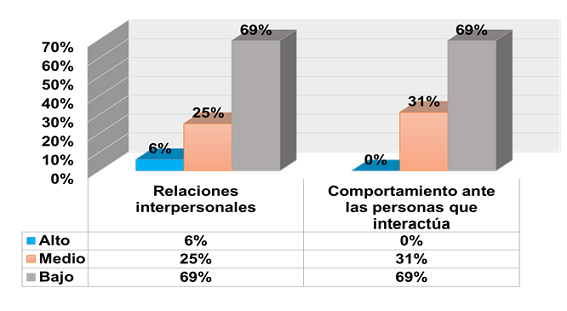
Fig. 5. - Results of the initial measurement applied to pregnant women in the social welfare indicator
The above aspects allow to state that in Physical Culture a program is needed that allows systematic and differentiated monitoring of the symptoms and clinical manifestations shown, oriented to the prescription in the biopsychosocial preparation for a satisfactory delivery in pregnant women with gestational diabetes and includes the participation of health facilitators committed to this task.
Proposal. Therapeutic physical activity program for pregnant women with gestational diabetes
General objective of the program: to improve the prescription in biopsychosocial preparation aimed at achieving a satisfactory delivery in pregnant women with gestational diabetes.
Stage 1. Preparation and adaptation.
General objective: prepare and adapt pregnant women towards the practice of therapeutic physical activities; as well as instructing them about gestational diabetes, pregnancy and the importance of systematically practicing physical exercises.
Specific objectives: instruct pregnant women on health education, determine their biopsychosocial characteristics, control blood glucose, incorporate the family in the support of interpersonal relationships and modes of action, improve mobility, circulation and strength, create correct postural habits, teach breathing- relax, adapt to physical load.
Duration: from pregnancy uptake (week 8-13).
Weekly frequency: five weekly frequencies.
Contents: Health education, warm-up, postural, respiratory and circulatory exercises, muscle relaxation, adapted yoga and walks.
Stage 2. Comprehensive therapeutic physical care.
General objective: improve prescription in biopsychosocial preparation aimed at achieving a satisfactory delivery in these pregnant women.
Specific objectives: increase mobility, maintain correct postural habits, practice prenatal stimulation, breathing and relaxation, strengthen muscles and joints of the pelvic floor, improve circulation, coordination skills, flexibility, endurance, psychosocial aspects, labor and shorten recovery time in the puerperium.
Duration: 14th. week of pregnancy to 37th. week (second and third trimesters).
Weekly frequency: five weekly sessions.
Contents: health education, postural, respiratory, circulatory exercises, relaxation, yoga, prenatal stimulation, flexibility and strength (pelvic floor), general strength, coordination (labor) and cardiorespiratory-metabolic resistance.
Structure methodology of therapeutic physical activity classes
Initial Part: consumption of food and water is explored to hydrate one or two hours before starting physical exercises and during them. Blood glucose self-monitoring. Pulse taking (PT) and TA. Warm-up at a slow pace. Lasts: 8-10 minutes.
Main Part: insulin is administered in areas little used or not in the exercises, due to its sensitivity during these, the dose decreases on the day of physical activity. She must drink water. PT. If the pregnant woman presents with hypoglycemia <3.8 mmol/L, she is offered sugary liquids. SCCDE, (2018). Physical exercises at a moderate pace. Duration: 25 to 30 minutes.
Final Part: recovery with slow walks combined with breathing and relaxation exercises. PT and TA. The effort gradually decreases. Post-exercise , the pregnant woman should drink sugary liquids to replace glycogen stores. Duration: 5 to 8 minutes.
Prescriptive components of therapeutic physical activities in the program:
(The prescription according to metabolic control, insulin, maternal age and pregnancy trimester).
Final result of the process of Therapeutic Physical Culture for pregnant women with gestational diabetes
Comparative results before and after the program for pregnant women with gestational diabetes in the dimensions, delivery evaluation and statistical processing (Table 1 and Table 2).
Table 1. - Evaluation of the indicators in the biological dimension
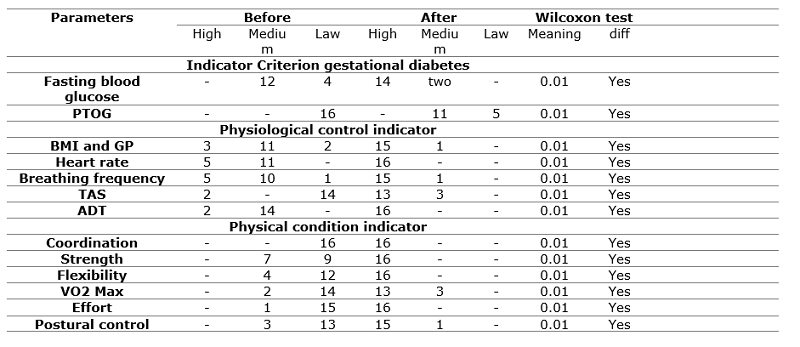
Legend: DS: significant difference
Table 2. - Evaluation of the indicators in the psychosocial dimension
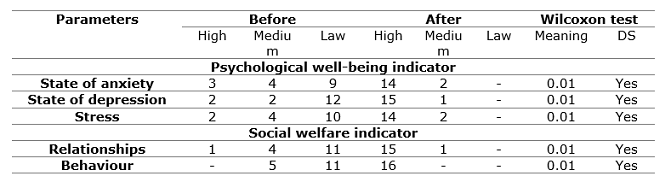
Legend: DS: significant difference.
When assessing the changes that occurred between the initial test and the final test in the biological and psychosocial dimension, they are significant, obtaining a result of 0.01 below the 0.05 value established for alpha; which denotes the effectiveness of the proposed therapeutic physical activity program for pregnant women with gestational diabetes. In statistical terms, the changes achieved show that the developed proposal revealed a significant incidence in these pregnant women, which favors the final evaluation; that is why the program is feasible to be applied for the benefit of the studied objective.
In the delivery evaluation, the 16 deliveries were observed; among the expected results for the breathing-relaxation management during contractions, it was evidenced that the parturient acted according to the stages of labor, used the types of breathing to achieve relaxation and adoption of antalgic positions in pain relief; which had a favorable influence on other parturient who were under the effect of stress caused by pain, responded correctly to the obstetrician's instructions in terms of relaxing, breathing and pushing at the right time, achieving effectiveness in pushing after having reached the maximum dilation. This evidences the coordination of the aforementioned motor acts and on which the non-prolongation of labor depends.
The presence of fatigue did not prevent the active attitude of the parturients when collaborating with the medical indications. They did not have prolonged deliveries. They report having saved their efforts during childbirth, since they did not perform unnecessary movements. There was better preparation on issues of pregnancy, childbirth, puerperium and gestational diabetes.
However, there were parturients who barely acted depending on the stages of labor they were going through, they barely used the different types of breathing; which had an unfavorable influence; in the end they managed to push with the help of the specialists. This led to prolonged labor. Fatigue made it difficult for the women in labor to cooperate only at times with medical indications. They had prolonged deliveries. They report having scarcely saved efforts during childbirth, by making unnecessary movements.
Regarding the types of delivery, involuntary and unconscious movements in facial muscles and during uterine contraction were shown in pregnant women. As labor progressed, no increases in the number and duration of involuntary and unconscious movements were shown. Maternal exhaustion did not prevent voluntary and effective maternal effort, endorsed by the non-instrumentation or Kristellier maneuver; they achieved a normal delivery without complications, the expulsion lasted 10-15 minutes. A laborious delivery lasted more than 15 minutes with symptoms, maternal exhaustion hindered voluntary and effective maternal effort, which led to instrumentation. A decision was made to perform a surgical delivery for failed induction of labor in a pregnant woman.
In metabolic and obstetric complications were not evidenced in 15 pregnant women and they maintained good metabolic control during delivery; however, one pregnant woman had a low birth weight baby. From these favorable results (Figura 6), the effectiveness of the therapeutic physical activity program applied to these pregnant women is evidenced, which together with the participation of all health facilitators allowed the achievement of a satisfactory delivery and contributed to the reduction of complications.
In general, it was determined that the therapeutic physical activities planned in the program and applied to pregnant women with gestational diabetes were effective in the evaluation of childbirth, by allowing the achievement of a satisfactory delivery with sufficient management of breathing and relaxation during contractions. in labor; as well as decreased metabolic and obstetric complications (Figure 6)
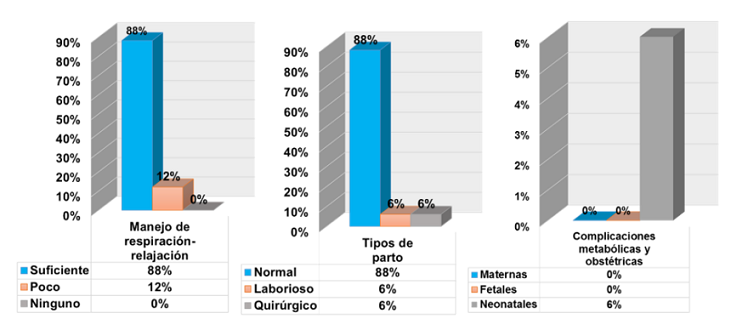
Fig. 6. - Results of the evaluation of childbirth performed on pregnant women with
gestational diabetes
Source: Rigol and Santiesteban, (2014); Wingert
et al, (2019); WHO, (2020).
In gestational diabetes, therapy is initiated through a special diet that allows the mother and the fetus to gain healthy weight without affecting glycemic levels, moderate physical exercise is recommended. If glucose remains elevated, insulin is added and glucose is monitored. (Cruz et al. and SCCDE, 2018); (Cruz et al., 2019). The bases of treatment according to Romero et al, (2018) are: diabetes education, nutrition, physical activity, self-control, medications, treatment of other conditions associated with pregnancy and specialized obstetric control.
The studies carried out by Días and Herrera, (2018), on gestational diabetes determined as fundamental pillars for its treatment: health education, diet, insulin administration and 30 minutes of physical activity 5 days a week; they helped the pregnant woman control glucose levels, relieved stress, improved heart, strength and flexibility, and decreased the chances of having type 2 diabetes in the future. Walking 30 minutes a day has shown benefits in maternal blood glucose levels in some studies, regular exercise during pregnancy is recommended by IND, (2017); ADA, (2018).
Training 3 days a week of moderate intensity 40-59 %, HR reserve and aerobic, strength, stretching, yoga and pelvic floor exercises for 140 minutes a week, improved insulin sensitivity and decreased insulin resistance. Being sedentary increases the chances of developing gestational diabetes (Davenport et al., 2018).
Physical exercise during pregnancy prevents excessive maternal weight gain by reducing the risk of gestational diabetes, without representing a risk to maternal and fetal well-being. The benefits are greater when the intervention includes combined exercises (Barakat et al., 2019).
CONCLUSIONS
The results obtained with the application of the program of therapeutic physical activities allowed to improve the prescription in the biopsychosocial preparation oriented to the achievement of a satisfactory delivery, showing favorable changes in the behavior of the pregnant women that favored their health, decreased the glycemic levels, the anxiety, depression and stress, in addition physiological control, good physical condition and a satisfactory delivery were achieved.
REFERENCES
American Diabetes Association. (2018). Prevention or delay of type 2 diabetes: standards of medical care in diabetes. Diabetes Care, 41 (Supplement 1), S51-S54. https://doi.org/10.2337/dc18-S005.
American Diabetes Association. (2021). Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes. Diabetes Care. 44(Suppl 1): S15-33. DOI: https://doi.org/10.2337/dc21-S002.
American College of Obstetricians and Gynecologists. (2018). ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstet Gynecol. 131(2): e49-64. PubMed.https://pubmed.ncbi.nlm.nih.gov/29370047/
Anuario estadístico de salud. (2021). Anuario estadístico de salud de Cuba 2020. La Habana. Cuba. https://salud.msp.gob.cu/disponible-edicion-49-del-anuario-estadístico-de-salud/Atención Primaria de Salud.
Anuario estadístico de salud. (2020). Anuario estadístico de salud de Cuba 2019. https:// www.salud.gob.cu/tag/anuario-estadistico-de-salud/&ved
Barakat, R., Refoyo, I., Coteron, J., e Franco, E. (2019). Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Brazilian journal of physical therapy, 23(2), 148-155. https://doi.org/10.1016/j.bjpt.2018.11.005
Cruz J, Llopis L, Lang J, González TM, González OJ, Ledón L. (2018). Atención al riesgo reproductivo de la mujer con diabetes mellitus en un municipio de la capital de Cuba. Rev Cubana Endocrinol. 29(2). 09/10/2021. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-29532018000200003
Cruz J, Márquez A. Jacinto Lang. (2019). La atención preconcepcional a la mujer con diabetes mellitus en Cuba. Rev Cubana Endocrinol.; 30(2):e169. 09/10/2021 http://www.revendocrinologia.sld.cu/index.php/endocrinologia/article/download/169/126
Davenport, M. H., et al (2018). Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. In British Journal of Sports Medicine 52(21) pp. 1367-1375. doi.org/10.1136/bjsports-2018-09935
Días Valdez, J., & Herrera Fraga, E. (2018). Uso del ejercicio físico con fines profilácticos en embarazadas. Anatomia Digital, 1(3), 15-23. https://doi.org/10.33262/anatomiadigital.v1i3.1050
Domínguez P, Domínguez J, Álvarez E, González A. (2016). Implicaciones del diagnóstico de diabetes gestacional en la salud futura de la mujer. Rev Ginecol Obstet Mex. 84(12):775-84. citado 09/07/2019 https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=73324
Fernández Baños, Raúl. (2016). Prescripción del ejercicio físico en sujetos con diabetes mellitus tipo 2 y diabetes gestacional RETOS. Nuevas Tendencias en Educación Física, Deporte y Recreación, (29), enero junio, 2016, pp. 134-139 Federación Española de Docentes de Educación Física Murcia, España. https://recyt.fecyt.es/index.php/retos/article/view/35130
Fernández, Y. et al. (2007). Programa Integral de Preparación Psicofísica para la embarazada (PIPPE). La Habana, Cuba: Instituto Nacional de la Diabetes. https://www.niddk.nih.gov/health-information/espanol/diabetes-gestacional-embarazada/publicationdetail.aspx
Organización mundial de la salud. (2020). Recomendaciones de la OMS Para los cuidados durante el parto, para una experiencia de parto positiva. Organización mundial de la salud https://extranet.who.int/rhl/topics/preconception-pregnancy-childbirth-and postpartum-care/care-during-childbirth/who-recommendation-companionship-during-labour-and-childbirth
Romero, R. F; Palomares L.; Delgado, L. G. (2018). Manejo integral de la diabetes durante el embarazo. Rev. Inf. cient. Sep-Oct; 97(5):1054-1064. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-99332018000200377
Rigol, O. y Santiesteban, E. (2014). Obstetricia y Ginecología. La Habana: Ciencias Médicas.
Vigil-De Gracia P, Olmedo J. (2017). Diabetes gestacional: conceptos actuales. Ginecol Obstet Mex. 85(6):380-390. Citado 09/06/2020. http://www.scielo.org.mx/pdf/gom/v85n6/0300-9041-gom-85-06-380.pdf
Wingert, A, Hartling, L, Sebastianski, M, Johnson, C, Featherstone, R. (2019). Clinical interventions that influence vaginal birth after cesarean delivery rates: Systematic Review & Meta-Analysis. BMC Pregnancy Childbirth. 30(19): 1-19. https://pubmed.ncbi.nlm.nih.gov/31888540/
Conflict of interest statement:
The authors declare that there are no conflicts of interest.
Authorship contribution:
The authors have participated in the writing of the paper and analysis of the documents.
![]()
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Copyright (c) 2022 Nadia Haydeé Sánchez
Rosabal, José Ezequiel Garcés
Carracedo, Lexy Lázaro Figueredo, Alexis Macías Chávez