
Revista PODIUM, May-August 2019; 14(2): 165-180
Translated from the original in spanish
Physical exercise guideline to counteract the osteoarthrosis´s morning syntoms in the elderly
Guías de ejercicios para contrarrestar los síntomas matutinos de la osteoartrosis en el adulto mayor
María Antonia Afre Socorro,1 Arelys de Armas Hernández,2 Danimary Labrador Afre2, Yariel Gener Rodríguez,2 Yosniel Benítez Falero3
1Universidad de Pinar del Río "Hermanos Saíz Montes de Oca".
Pinar del Río, Cuba. E-mail: leinad.labrador@inder.cu
2Hospital General Docente "León Cuervo Rubio"
de Pinar del Río. Pinar del Río, Cuba. E-mail: danimaryla@gmail.com
3Hospital General Docente "Abel Santamaría Cuadrado"
de Pinar del Río. Pinar del Río, Cuba.
Received: March 28th, 2019.
Accepted: April 30th, 2019.
ABSTRACT
Attention to the elderly is one of the priorities of the Cuban government. The research was carried out in the doctor´s office number 6 of Pinar del Río municipality. Theoretical methods were used (review of documents, inductive-deductive) and empirical methods (observation and interview) that made possible to deepen into the elderly characteristics, more common diseases, symptomatology and treatments, what confirmed that the elderly, when awakening, suffer from greater symptomatology in some diseases. Some guides of physical exercises were made to compensate this disorder, which are mainly based on joint mobility. The exercises are simple and easy to remember. Favorable results have been obtained according to the sample selected for the study, it was achieved pain relief and reduction of numbness, as well as undoubtedly a better day start with a favorable mood.
Keywords: the elderly; osteoarthrosis; guide of physical exercises; joint mobility.
RESUMEN
La atención al adulto mayor es una de las prioridades del gobierno cubano. La investigación se realizó en el consultorio 6 del municipio Pinar del Río. Se utilizaron métodos teóricos: (revisión de documentos, inductivo-deductivo) y empíricos: (observación y entrevista) que permitieron profundizar en características de los adultos, enfermedades más comunes, sintomatología, tratamiento, lo que posibilitó constatar que los adultos mayores, al despertar, presentan mayor sintomatología en algunas enfermedades. Para atender este caso, se elaboraron guías de ejercicios para compensar este padecimiento. Estas guías se basaron, fundamentalmente, en el trabajo con la movilidad articular. Los ejercicios son sencillos y fáciles de recordar. Se han obtenido resultados favorables respecto a la muestra seleccionada para el estudio, se logró alivio en los dolores y reducción del entumecimiento y un mejor inicio del día, con un favorable estado de ánimo.
Palabras clave: adulto mayor; osteoartrosis; guía de ejercicios; movilidad articular.
INTRODUCTION
The United Nations refers to the older adult as a person who has turned 60 or over, although there is no clear consensus on this since some countries take 65 as the lower limit and others even set 70 as the norm. González, A. and Vázquez, I. (2010)
Scientific and technological advances in medicine have reduced fatal diseases and made it possible to reduce the mortality rate and increase life expectancy. As a result, society at the end of the twentieth century was faced with a new phenomenon: the longevity of its population.
It is now widely acknowledged that the impact of disease on patients cannot be fully described by objective health measures such as the spread of a tumour, the result of a biopsy or the measurement of blood pressure; other "subjective" factors such as pain, functional capacity or emotional well-being have to be considered. Hootman, J. and others (2018)
Osteoarthrosis (OA) or osteoarthrosis is the most common joint disease in the adult population and is currently a major public health problem. Peat, G. and others (2001)
Epidemiological studies on osteoarthrosis show important methodological variations according to the criteria used for diagnosis; radiological criteria tend to overestimate the disease and the most commonly used diagnostic combination is the association of clinical and radiological criteria. Osteoarthrosis causes chronic pain and incapacitates the patient. It is the most common rheumatic disease, characterized by a progressive decrease in articular cartilage, with destruction of the subchondral bone of the joint, and inflammatory phenomena may be associated with its evolution. Joint pain is progressive, accompanied by stiffness and loss of joint function, nocturnal pain is common and can trigger it with minimal movement, in the advanced stages of the disease. The symptoms and signs of the disease are limited to the affected joint, but if it is polyarthy-cular it can simulate a systemic inflammatory disease.
Other research showed that women had up to 26 % OA in their hand, compared to 13% of men in the Framingham cohort. Bilateral symptoms were observed in 16% of women and 7% of men. The joints with the greatest radiological affection were the distal interphalangeal joints. OA in hands caused functional disability in activities of daily living such as carrying lumps, grasping small objects and writing. Olsen C. F. and Bergland, A. (2014).
There are currently studies demonstrating differences in prevalence between different populations. There is a low prevalence of hip OA in a Chinese population compared to a similar population in the United States, as well as a high percentage of lateral knee space impairment in a Beijing population compared to this impairment in the Framingham population in the United States. Kemmler, W. (2015)
In the early diagnosis of osteoarthritis, known risk factors, which predispose to the onset of the disease, may be useful, general and local and, in turn, modifiable and non-modifiable. Felson, D.T. (2004)
General risk factors that cannot be modified:
Modifiable general risk factors:
Local risk factors.
Any eventuality that alters the geometric congruence of the articulation will mean a favourable factor for the development of osteoarthritis. We can quote:
The amplitude of joint movements varies by age, sex, and race. Limitation of active mobility may be due to joint pathology, while passive mobility expresses joint disease. The range of joint mobility is measured using the "Zero Method", where the anatomical position of the trunk and limbs is considered as zero degrees. Joint stability may be compromised in ligamentous disorders. Varahra, et al., (2018)
In the rheumatology manuals, clinical-pathological correlations appear on the origin of pain in osteoarthritis and thus the possible structures are all the joints and periarticular that present innervation: bones (increased intraosseous pressure, microfractures, periosteal elevation), synovial and bursas (effusion, synovitis), nerves (pressure of the osteophytes on neighbouring nerves), periarticular structures (ligaments, muscles), meniscus lesions, etc. It is difficult, in clinical practice, to know which of these structures is the cause of pain in the patient, since it is more an approach and an art than a science.
The best way to get to know your cause is a thorough clinical examination, and probably the most affordable imaging technique that can help is ultrasound. In studies that have sought an association between pain and osteoarthritis, the following factors have been detected: sex, age, lower limb involvement, obesity, psychological factors such as anxiety and depression, joint effusion, Baker's cyst. The intensity of the radiological grade also correlates with an increase in the probability of perceiving pain, although patients with severe radiological affectation may be asymptomatic. Mendieta, E. (2005)
The progression of the disease is usually slow. The best studied location is the knee and long-term studies show that progression occurs in one-third to two-thirds of patients, while a significant percentage of them may remain in a relatively stable condition. Bjordal, et al. (2004)
The treatment of osteoarthritis is fundamentally symptomatic and has three priority objectives: to relieve pain and discomfort; to improve the functional capacity of the affected joints; and to slow the progression of the disease. The treatment is based on pharmacological and non-pharmacological measures in addition to surgical treatment. Prolonged immobilisation is not recommended as it favours the progression of osteoarthritis.
Physical therapy plays a fundamental role in the management of osteoarthritis and its objectives are to reduce joint pain and stiffness, maintain and promote muscle strength and trophism, and improve joint mobility and biomechanics. It uses techniques such as thermotherapy, hydrotherapy, massages and a physical exercise program adapted to each situation. Rodríguez and others, (2017). Exercise has been shown to be beneficial in pain control and in the functionality of the knee and hip with OA. All types of exercise that help strengthen periarticular muscles have proven useful. It is important to insist that the patient carry out some type of physical activity, as it is known that OA predisposes, due to pain, to less exercise, which results in an increase in cardiovascular morbidity and mortality. Park, et al. (2017)
The patients with osteoarthritis have loss of strength mainly in the muscular groups of the affected articulations, reason why it is useful the accomplishment of exercises that strengthen the musculature and improve the joint mobility, when strengthening the muscular force diminishes the overload, at the same time that diminishes the degree of anxiety and depression as a consequence of the improvement of the physical capacity.
Exercises must be carried out when there is no pain, in a suitable environment, with comfortable clothes that allow certain flexibility. It will be done correctly, when the pain has disappeared and will be suspended if it reappears. You will rest between exercises and these will increase in number and intensity. (Moreira, Oliveira, Lirani-Galvão, Marin-Mio, Santos and Lazaretti-Castro, (2014)
In view of the above, the following scientific problem is proposed for the study: how to counteract the morning symptoms of osteoarthrosis in the elderly in medical practice number six, ¿belonging to the “Pedro Borrás” health area of the municipality of Pinar del Río?
In order to respond to this problem, the following objective was set: To elaborate exercise guides to counteract morning symptoms related to osteoarthrosis in the elderly in medical office number six, belonging to the "Pedro Borrás" health area, in the municipality of Pinar del Río.
MATERIAL AND METHODS
A quasi-experimental epidemiological investigation was carried out, consisting of a proposal for exercise guides to be used, upon awakening, by older adults with degree of validity I (adults capable of taking care of themselves in their daily activities at home and in the community) and II (adults who have no social life, but have adequate family and individual life), with symptoms of suffering from osteoarthritis.
For the initial diagnosis, a work was carried out with the document Historia de salud familiar (Family Health History), from medical practice number six, from the health area "Pedro Borrás", belonging to the municipality of Pinar del Río, which made it possible to select the sample according to its pathology; in addition, an interview was carried out with older adults that allowed us to know their sufferings and determine their needs. The older adults interviewed signed their informed consent. Inclusion and exclusion criteria were taken into account.
Inclusion criteria:
Exclusion criteria:
Taking into account the theoretical study carried out and the results of the scientific methods used, an inventory of difficulties and potentialities was made:
Difficulties:
Potentialities:
RESULTS
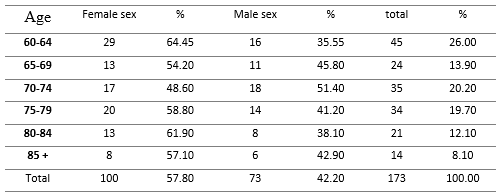
Next, the results obtained in the initial diagnosis will be analyzed in order to characterize the current situation of the older adults selected for the study. In chart 1, it can be observed that in the sample studied, women predominate over men (57.80 % and 42.20 % respectively). The most frequent age range was 60-64 years for the female sex and 7074 years for the male sex. This is in correspondence with foreign and national epidemiological studies, since it is known that women tend to live a little longer, due to the cardioprotective effect of female hormones. (Table 1)
Table 1. - Age distribution of older adults in medical practice number six
in the "Pedro Borrás" Health Area. Pinar del Río, 2018
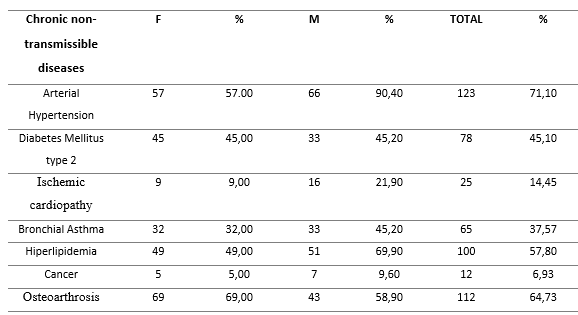
In the clinic, osteoarthrosis was the second most common chronic noncommunicable disease in older adults after hypertension with 64.73 %, although it is considered to be under-recorded. (Table 2)
Table 2. - Chronic non-transmissible diseases in the elderly of the medical office number six
of the Health Area "Pedro Borrás". Pinar del Río, 2018
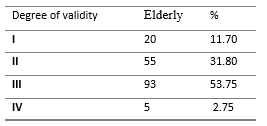
In the doctor´s office, older adults predominate with degree of validity III, they can meet their individual needs, but are not able to maintain an adequate individual family life. Adults from groups I and II were selected for the study, so from a universe of 75 adults, they were selected for having symptoms of osteoarthrosis 35, representing 46.66 %. (Table 3)
Table 3. - Degree of validity of the older adults of the medical practice number six
of the Health Area "Pedro Borrás". Pinar del Río, 2018
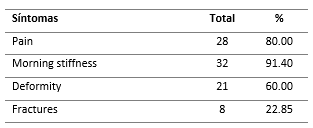
Among older adults identified with osteoarthrosis, the most frequently reported symptom was morning stiffness (91.40 %), followed by pain (80.00 %), in accordance with the reported literature, and it is time to awaken when these symptoms become more acute. (Table 4)
Table 4. - Symptoms associated with osteoarthrosis in elderly, from medical practice number six in the
"Pedro Borrás" Health Area. Pinar del Río, 2018
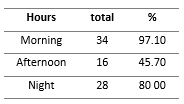
It was found that the morning schedule, specifically upon awakening, is the one in which the symptoms of osteoarthrosis were most annoying (97.10%), mainly rigidity and subsequent pain, in line with the literature reviewed. (Table 5)
Table 5. - Time of day with aggravation of symptoms related to osteoarthrosis in older adults,
from doctor's office number six
of the Pedro Borrás Health Area. Pinar del Río, 2018
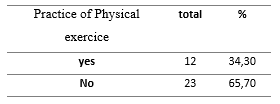
The highest percentage of elderly interviewed stated that they did not exercise, 65.70 %. They exemplified exercises such as going out to buy food, carrying out household chores and incorporating grandparents into the circle to a lesser extent. (Table 6)
Table 6.- Practice of physical exercises for older adults, from doctor's office number six
in the "Pedro Borrás" Health Area. Pinar del Río, 2018
Taking into account the results found and the need for elderly to alleviate the symptomatology of osteoarthrosis they suffer, two exercise guides were elaborated to alleviate the morning symptoms of this nosological entity.
Two exercise guides were elaborated
The first guide has 16 exercises and some orientation about them, all on one sheet, with good font size. The aim is not to overwhelm the adult with a lot of explanations and try to encourage him in his realization. Although they are told that a month they will be given another guide, this will only be done if the adult refers to remember all the exercises and perform them with ease.
The second guide has 17 exercises. There are exercises that do not vary from one guide to another, but this includes some that require a little more coordination.
Characteristics of the proposed guides and the exercises that compose them:
With no more important aspect to communicate, the exercise guides are shown below.
Exercise Guide 1
The exercises described below should be performed upon awakening, in bed, at a slow pace and 6 to 15 repetitions, as follows:
1. First week six repetitions.
2. Second and third week eight repetitions.
3. Fourth, fifth and sixth week 12 repetitions.
4. Next weeks 15 repetitions.
From sitting on the edge of the bed perform:
These exercises must be performed daily, you can start them with your eyes closed (after you know them) No matter the order in which they are performed, it is recommended to start them lying down. This is a way to start the day with greater mood, activating organs and systems, relieving pain and joint stiffness that they present upon awakening.
These exercises do not replace the classes of the older adult.
Exercise Guide 2
After some time doing the exercises oriented in the previous guide, they are given a new group of exercises as easy and simple as the previous ones, hoping that they will help them to maintain or improve their organic functions and that the pains and numbnesses are relieved by so many hours of inactivity by sleeping. These exercises will be carried out from 8 to 15 repetitions.
Raise one leg bent at the knee, with the help of the hands and with these bent, extend and rub the toes and ankles.
Do the exercises every morning when you wake up, do them, they are for your physical and mental well being, do not forget that physical activity relieves all evils.
In a conclusive way, it is stated that through this research it is corroborated that in the studied sample women between 60 and 70 years old predominate as an age group and osteoarthrosis is the second most frequent chronic non-transmissible disease after arterial hypertension.
The most frequent symptoms related to osteoarthrosis in older adults reported were morning stiffness and pain, with higher prevalence of the same at the time of awakening. It was identified that the highest percentage of older adults interviewed did not engage in physical exercise. Exercise guides to alleviate the morning symptoms of osteoarthrosis were developed for implementation in the near future and evaluated in later researchs.
BIBLIOGRAPHIC REFERENCES
Bjordal, J.M., Ljunggren, A.E., Klovning, A. y Slørdal, L. (2004). Non-steroidal anti-inflammatory drugs, including cyclo-oxygenase-2 inhibitors, in osteoarthritic knee pain: meta-analysis of randomized placebo controlled trials. BMJ., 3 (29), pp13-17. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/15561731
Figueroa, M., Andreu S. (1996). Manual de enfermedades reumáticas de la Sociedad Española de Reumatología. Madrid: Editorial Mosby/Doyma Libros S.A.
Felson, D.T. (2004). Risk factors for osteoarthritis: understanding joint vulnerability. ClinOrthopRelat Res.,4(27), pp16-21. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/15480060
González, A., Vázquez, I. (2010). Calidad de vida relacionada con la salud en adultos mayores de una clínica de medicina familiar. RevMedInstMex Seguro Soc, 48 (5), pp 475-484. Recuperado de: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=37373
Hootman, J.M., Murphy, L.B, Omura, J.D., Brady ,T.J., Boring, M., Barbour, K.E. y Helmick CG. (2018). Health Care Provider Counseling for Physical Activity or Exercise Among Adults with Arthritis en United States. Morb Mortal WklyReport, 66 (5152), pp 1398-1401. doi: 10.15585/mmvr.mm665152a2. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/29300722
Huber, J., Dieppe, P., Dreinhoefer, K., Günther, K.P. y Judge, A. (2017). The Influence of Arthritis in Other Major Joints and the Spine on the One-Year Outcome of Total Hip Replacement: A Prospective, Multicenter Cohort Study (EUROHIP) Measuring the Influence of Musculoskeletal Morbidity. J Bone JointSurg Am. 99 (17), pp 1428-1437. doi: 10.2106/JBJS.16.01040 Recuperado de : https://www.ncbi.nlm.nih.gov/pubmed/28872524
Kemmler, W., Bebenek, M., Kohl, M.yvon Stengel, S. (2015). Exercise and fractures in postmenopausal women. Final results of the controlled Erlangen Fitness and Osteoporosis Prevention Study (EFOPS). OsteoporosInt., 26(10):2491-9. doi: 10.1007/s00198-015-3165-3. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/25963237
Mendieta, E.M. (2005). Relevancia de los hallazgos clínicos y radiológicos en la artrosis. RevEspReumatol., 32(1), pp 37-41. Recuperado de: https://www.elsevier.es/es-revista-revista-espanola-reumatologia-29-articulo-relevancia-los-hallazgos-clinicos-radiologicos-13071163
Moreira, L.D., Oliveira, M.L., Lirani-Galvão, A.P., Marin-Mio, R.V., Santos, R.N. y Lazaretti-Castro, M. (2014). Physical exercise and osteoporosis: effects of different types of exercises on bone and physical function of postmenopausal women. Arq Bras EndocrinolMetabol., 58 (5), pp 514-22. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/25166042
Olsen C.F. & Bergland, A. (2014). The effect of exercise and education on fear of falling in elderly women with osteoporosis and a history of vertebral fracture: results of a randomized controlled trial. Osteoporos Int., 25 (8):2017-25. doi: 10.1007/s00198-014-2724-3. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/24807628
Park, K.S., Yoo, J.I., Kim, H.Y., Jang, S., Park, Y. yHa, Y.C. (2017). Education and exercise program improves osteoporosis knowledge and changes calcium and vitamin D dietary intake in community dwelling elderly. BMC Public Health., 17 (1): p 966. doi: 10.1186/s12889-017-4966-4. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/29258608
Peat, G., McCarney, R., Croft, P. (2001). Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann Rheum Dis.; 60 (2), pp 89-90. Recuperado de: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1753462/
Rodrigues, I.B., Adachi, J.D., Beattie, K.A. yMacDermid, J.C. (2017). Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMCMusculoskeletDisord., 18 (1), p 540. doi: 10.1186/s12891-017-1914-5. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/29258503
Varahra, A., Rodrigues, I.B., MacDermid, J.C., Bryant, D., Birmingham, T. (2018). Exercise to improve functional outcomes in persons with osteoporosis: a systematic review and meta-analysis.OsteoporosInt. 29 (2), pp 265-286. doi: 10.1007/s00198-017-4339-y. Recuperado de: https://www.ncbi.nlm.nih.gov/pubmed/29306984
![]()
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International license
Copyright (c) 2019 María Antonia Afre Socorro