
Revista PODIUM, September-December 2019; 14(3): 372-391
Translated from the original in spanish
Older adult systematic practitioner: tests to assess your physical condition
El adulto mayor practicante sistemático: pruebas para evaluar su condición física
Leidys Escalante Candeaux,1 Manuel Medina Álvarez,1 Hermenegildo José Pila Hernández,1 Annia Gómez Valdés4
1Universidad de Ciencias de la Cultura Física "Manuel Fajardo" (UCCFD). La Habana,
Cuba. E- mail: leidymyy@inder.cu ; drpila@inder.cu
2Universidad de Pinar
del Río "Hermanos Saíz Montes de Oca", Departamento de Ciencias Aplicadas. Pinar del Río,
Cuba. E-mail: annia.gomez@upr.edu.cu
Received: April 1st, 2019.
Approved: August 30th, 2019.
ABSTRACT
In Cuba, attention to the Elderly Programme is a priority and physical activity professionals working in this pedagogical field are aware of it. Systematic practitioners of older adults are encouraged to enhance their functional independence, taking into account work with all the physical capacities involved in motor actions. The main objective of the research was to create an instrument that would allow the evaluation of the physical condition with its corresponding methodology, which would allow to increase their quality of life from the improvement of their functional state. In addition to providing the rules to plan a differential work that took into account the differences of sex, age and chronic diseases nontransmissible to the practitioner as an important complement to the battery developed. The program was aimed at older adults who practice physical exercise at least three times a week. The materials used correspond to metric tape, cones, chalks, chairs and weights of 8 kilos for men and five for women. The methods and techniques used were: survey, interview, observation and measurement. With the results of the physical condition assessment, teachers will be able to plan their work better and older adults who are systematic practitioners will benefit from optimal care as they can be attended to in a differentiated manner. In this opportunity the battery is being socialized and its methodology only, the norms for the evaluation will be reason for another article.
Keywords: older adult; physical condition; physical tests.
RESUMEN
En Cuba, la atención al Programa del Adulto Mayor está priorizada y los profesionales de la actividad física, que se desempeñan, en esta esfera pedagógica, están conscientes de ello. Con los adultos mayores, practicantes sistemáticos, se promueve potenciar su independencia funcional, teniendo en cuenta el trabajo con todas las capacidades físicas, implicadas dentro de las acciones motrices. El objetivo principal de la investigación fue crear un instrumento que permitiera la evaluación de la condición física con su correspondiente metodología, el cual permitiera incrementar su calidad de vida, a partir del mejoramiento de su estado funcional. Además, de proveer las normas para planificar un trabajo diferencial que tuviera en cuenta las diferencias de sexo, edad y las enfermedades crónicas no trasmisibles del practicante, como complemento importante de la batería elaborada. El programa estuvo dirigido a aquellos adultos mayores que practican ejercicios físicos, como mínimo, tres veces a la semana. Los materiales empleados se corresponden con cintas métricas, conos, tizas, sillas y pesas de 8 kilos para los hombres y de cinco para las féminas. Los métodos y técnicas empleados fueron: la encuesta, la entrevista, la observación y la medición. Con los resultados de la evaluación de la condición física, los docentes podrán planificar mejor su trabajo y los adultos mayores, practicantes sistemáticos, se beneficiarán con una atención óptima ya que podrán ser atendidos de manera diferenciada. En esta oportunidad, se está socializando la batería y su metodología solamente; las normas para la evaluación serán motivo de otro artículo.
Palabras clave: adulto mayor; condición física; pruebas físicas.
INTRODUCTION
In Latin America, from 48 million older adults in 2005 (8.8 %) to 114.5 million in 2030 (16.3 %). Statistical projections in developing countries show that the growth of the population over 60 years of age is faster than in developed countries. Guerrero and Yépez, (2015).
In Cuba, an increase of 450,000 older adults is forecast for the year 2025, rising to 2.9 million people aged 60 or over.
It coincides with (Rubio et al., 2015) that the aging population of the world and of Cuba is a demographic phenomenon associated with the scientific-technical revolution of the 21st century. It ranks among the oldest countries in Latin America and the Caribbean; without a doubt, the aging of our population must be considered the result of the success of our society, but it is still a governmental and institutional concern. Martínez et al., (2018) and, in correspondence with these authors, should also be a socio-family concern. Varela-Pinedo et al., (2015)
This is the most vulnerable population group in our society and will require specific care criteria, an increase in expenses for care and attention not only in public institutions, but also in the family, creating complex situations that will require more dynamic solutions, both in their structure and in their functioning. The universe of older adults, due to their education, lifestyles, roles played and other factors, will demand - and are already demanding - a more intense and different qualitative attention in the different social spheres.
The health of older adults, who are aware of their limitations, the product of age and social stereotypes about old age, taking into account their conceptions of what it means to them, is changing. Vargas et al., (2017)
Buitrago et al., (2016) quoting Hidalgo, refers that,
"The aging process acts in a similar way to inactivity, producing effects similar to those caused by sedentary life and, if we add to this the fact of not carrying out any physical activity (70% of the population is sedentary), the risk will be greater". Older adults, in this period, experience numerous bio psychosocial changes that depend on lifestyle, social system and family and continuously influence the various areas of operation Loredo-Figueroa et al., (2016).
Society strives to ensure that older adults are independent people, capable of carrying out by themselves the greatest number of motor actions, of remaining active, who can make decisions at the end of their days in the fullness of their form, both psychically, physically and socially.
They have the right to receive the benefits necessary for their integral attention; to this end, access to medical services, orientation regarding their health, nutrition, hygiene and all those aspects that favor their personal care are included (López, 2018). In line with the above, add the physical socializing activities par excellence, in addition to improving their practices of daily life.
Sport is one of the activities that is carried out under the influence of changes and it could be said that we are living in accelerated times. People aged 60 or over may be the group where the need for this activity is most felt because they discover the benefits of physical activity, sports, martial arts, basic gymnastics and participation in gymnastic compositions, dance and dance classes, walking, swimming, bicycling, and going to the gymnasiums and areas where the bio-healthy are located as a new community alternative.
The reasons are diverse. Most of the authors agree that adults demand physical activity for the following reasons: To compensate for the lack of physical activity in everyday life, to live more satisfactorily, to achieve self-acceptance and personal esteem, to prevent and successfully treat physical and mental illnesses, to increase social relations and to occupy leisure time, because according to Cuellar et al., (2016) "the regular practice of some physical activity helps to maintain the independence of the older adult".
There is a negative change associated with retirement. Most people, when they retire, become accustomed to a sedentary regime when they cease the obligation to move from their homes to the workplace. Many of them have been physically active at work and begin to adapt to other sedentary domestic actions, which contribute to the emergence of obesity and, with it, other diseases.
It is significant that the male persons, in these ages, are incorporated much less to the physical activities, in spite of their importance, of the benefit that they provide by the indisputable improvement of their physical capacities and, therefore, in the functional thing, the restoration of the human relations and, among other aspects, the elevation of their self-esteem, of the hope of a worthy old age, all which entails a notable improvement in their quality of life.
With systematic physical activity, the elderly can guarantee the basic activities of daily life: bathing, dressing, eating, combing their hair on their own; the instrumental ones: carrying out domestic tasks, shopping, travelling, attending various social activities and the advanced activities of daily life, and i.e. carrying out sporting activities.
For Chan (2015), active ageing is the process of participation, integration and security in order to improve the quality of life and, therefore, her physical condition as she ages. Action is needed in multiple sectors to ensure that these people remain a resource for their families, communities and economies.
For this reason, the professionals of Physical Education for adults insist on the systematic practice of organized, dosed and planned physical activities in order to provide them with quality from the functional point of view (Escalante, 2015) that coincides with the previous author, who points out that it is not only the evaluation of physical and mental capacities that must be determined, but also the interactions with the environments that inhabit throughout life.
It is also argued that, in old age, the elderly are burdened with fears, worries, anxieties and myths, hence physical activities improve communication, expression and socialization with their environment and even play at those ages plays a physical, social and cultural role. Aging is not synonymous with a sedentary and routine life; on the contrary, aging can be a stage full of vitality if it is so proposed. Giai, (2015), therefore, limitations in the execution of daily activities represent a serious problem for the elderly, since they are an indicator of risk for the health of the individual and directly affect his quality of life, according to Quino et al., (2017).
Gymnastics classes for older adults and the evaluation of their physical condition are aimed at the fuCNTDSional as a dynamic and structured process, in order to know what a person is capable of and not just, what he or she is incapable of. This allows guaranteeing the adequate use of free time, to diminish the indexes of risk factors by means of the systematic design of varied activities that increase the quality of life from an improvement of their self-esteem and fuCNTDSionality.
Establishing indicators that make this evaluation possible is the purpose of this research, as this is a subject that is not dealt with much in the literature. With the results of the proposed evaluation, teachers of community physical activity will achieve a better planning of their work and older adults, systematic practitioners, can be served in a differentiated way, which will increase their autonomy, independence and fuCNTDSionality, in order to maintain health and achieve a better quality of life, which entails a state of complete physical, mental and social well-being.
MATERIALS AND METHODS
The methods and techniques used were survey, interview, observation and measurement. The battery is structured in seven (7) tests, which general objective was the evaluation of the physical condition in older adults, systematic practitioners, in Cuba, by age groups, sexes and the individual diagnosis by base disease and with the results of the investigation the corresponding national norm was established, tempered to their conditions. (Figure 1)
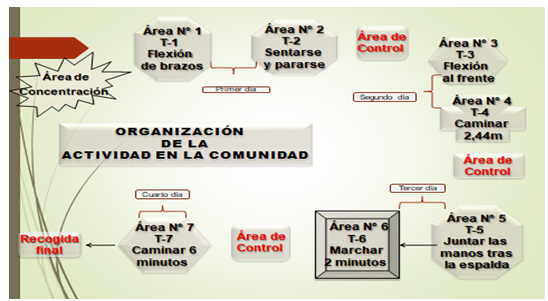
Fig. 1 - Organization of work to apply the battery of physical tests
The battery is based on the principles of active aging, which constitutes a regularity within the process, ensures a close interrelationship in physical activity and facilitates the creation of contexts. The practitioner, according to his particular characteristics, collaborates in the process and at the same time feels supported; to the same extent, he satisfies his needs because there is agreement between the demands of this activity and its real possibilities.
According to Varela, (2016), the World Health Organization (WHO) considers active aging as the process of optimizing opportunities for health and participation. It is a state where an individual is able to invoke adaptive psychological and social mechanisms to compensate for physiological limitations and thus achieve a sense of well-being, self-evaluation and a sense of personal fulfillment.
On the other hand, from a purely scientific angle, "The theory of organs and system" supports the need for population stratification and standards for basic age, gender and chronic non-transmissible disease (NCD) assessment; in essence, it justifies the differences in the dynamics of ageing and the relevance of the proposal.
For Beratarrechea, (2016), Integrated Geronto-geriatric assessment (IGV) is a multidimensional diagnostic process to determine the health problems of older people from the point of view (...) of diseases, such as: arterial hypertension, diabetes mellitus, bronchial asthma and obesity, which in the elderly are presented, and for this, it is recommended to change lifestyles, which from the physical point of view contribute to mobility and ability to perform, autonomously, activities from the psychosocial.
Including more actors would contribute to a multi and interdisciplinary vision around the same phenomenon that goes beyond an age and, on the other hand, manifests itself throughout the course of life. Therefore, the vision of a greater number of disciplines is indispensable and useful for this purpose. Gutierrez and Kershenobich, (2015)
The fundamentals of ageing demonstrate that degenerative processes at that stage of life prevail over regenerative processes and are expressed in the gradual, orderly and continuous transformation of the organism, both morphologically and physiologically and psychosocially, which implies quantitative, progressive, irreversible and unrepeatable changes and increasing complication in each person because of ageing processes.
From the functional point of view, the loss of adaptability is given by a decrease in the reserves in the tissues, which causes the inability of the body's homeostatic systems to combat the fluctuations of the outside world and maintain, in an adequate manner, the internal environment.
The categories that are declared are identified with the capacities to evaluate in each one of the tests, in these they are related the force and the flexibility for both hemibodies, the dynamic balance like ability within the coordinating capacity and, finally, the aerobic resistance. The chronic non-transmissible diseases considered for this study - bronchial asthma, obesity, diabetes mellitus and arterial hypertension - are the most frequent in the older Cuban population and considering them constitutes an essential aspect that allows planning and organizing the teaching process with greater possibilities of success.
From the philosophical point of view, it is an approach to reality whose pedagogical purpose penetrates more and more into the essence of Physical Education for the elderly, through the stimulation of their physical potentialities.
From the social point of view, this research responds to the real needs of our population, in the historical and geographical context; consequently, the evaluation of the physical condition in these ages is directed towards the solution of the problem detected in social praxis.
From the psychopedagogical angle, it is a fundamental component of the system of actions that takes into account the coordination and fluidity of movements, it is a way of organizing and regulating the activity directed to the achievement of the basic objective: to optimize the potentialities and the functionality by means of the integrated development of physical capacities and motor abilities, in correspondence with its diverse characteristics. The mediating role of the teacher is conceived, with methodological orientations for the application of the battery of tests since it is conceived in such a way as to favor a pedagogical and transforming action of these specialized teachers and the maintenance or effective functional change in the quality of life of the elderly adult.
Tests to assess the physical condition of the older adult systematic practitioner
Test #1. Getting in and out of a chair in 30 seconds
Objective: to assess the behavior, physical capacity, endurance, strength of the lower extremities in older adults, systematic practitioners.
Theoretical basis: strength at these ages is a reliable marker of the state of health and well-being of people and the maintenance of muscle tone, in the legs, is related to the reduction of falls and bone fractures.
Procedure
Position: standing with legs apart, arms crossed at chest, in front of a chair, with backrest glued to the wall for greater safety.
Task: sitting and standing, without back support. Repeat the action at an appropriate pace.
Time: 30 seconds.
Means and instruments: chair with seat 46 cm. from the floor and stopwatch.
Indication: make previous demonstration of what the older adult must do.
Test #2. Forearm Flexion and Extension, with Weight (Left and Right)
Objective of the test: to evaluate the resistance of the upper extremities in older adults, systematic practitioners.
Theoretical foundation: instrument aimed to diagnose the resistance force in the upper planes, in the population being studied; it is an indicator of quality and independent life expectancy, which qualifies if the older adult has the need for external help.
Procedure
Position: seated with support and back straight and care is taken not to hit the hand with the chair. Keep the arm extended to the side of the body as close as possible. The other arm should rest on the corresponding thigh. Repeat the action with the other arm.
Task: bend and extend the arm with the implement.
Time: thirty seconds (the two movements are considered as an exercise and the collaborator counts the repetitions, in an internal way).
Indication: make previous demonstration of what the older adult should do.
Means and instruments: Weights of 2.5 kg for women and 4 kg for men, chair and stopwatch.
Test #3. Get up, walk 2.44 m and sit again
Objective of the test: to assess agility and dynamic balance in older adults, systematic practitioners.
Theoretical basis: to know the possibilities of each older adult for maintaining balance and agility in old age; this provides greater postural stability, improves their motor skills to perform their basic activities, promotes balance and reduces the risk of falls.
Procedure
Position: sitting on the edge of a chair, with the back attached to the wall and in front of it eight steps will be marked on the floor.
Task: at the given order, the older adult gets up, walks to the mark at 2.44m., turns around, returns and sits, the seconds are counted in going and returning.
Time: if the person is delayed in getting up does not matter, the time is measured from the moment the person gets stand, measure only the time of the exercise. Perform the exercise next to the grandfather as a safety measure.
Indication: make previous demonstration of what the older adult should do.
Means and instruments: chair, chalk or adhesive tape to mark the floor and stopwatch.
Test #4. Bending of the trunk to the front
Objective of the test: to evaluate active flexibility.
Theoretical foundation: it is one of the first qualities to be affected over the years. Exercises aimed at minimizing these effects improve joint mobility and range of motion.
Procedure
Position: Sitting on the edge of a chair with one leg flexed and the dominant leg extended with the heel resting on the floor.
Task: inhale and carry arms extended above, with one hand on top of the other and fingers together, exhale when flexing the trunk forward, to touch or surpass the toe with the toes, maintain the stretching position. The distance between the tip of the toes and those of the hands should be measured: if it is exceeded, it is considered positive, otherwise it is negative.
Time: hold position for two seconds.
Indication: to exonerate individuals suffering from osteoporosis and to carry out a previous demonstration of what the older adult should do.
Means and instruments: tape measure or wooden ruler and a chair.
Test #5. Perform two minutes of walking in place
Objective of the test: to evaluate the resistance to strength in the lower extremities.
Theoretical basis: This is a capacity that depends, largely, on the adequate transport of oxygen and nutrients on a direct relationship between respiratory coordination and cardiovascular health.
Its practical applications are the amplitude, direction and rhythm of the strength involved. The relationship between force and time is the central component of motor programming and has important implications for motor control.
Procedure
Position: standing sideways, with right hand resting on a column, post or wall. With the tape measure, measure the distance between the knee and hip, bend in half and mark that height on the wall.
Task: march and raise the knees to the height of the mark made on the wall, the collaborator will bend down to observe that the knee reaches the height of the mark and stimulate the adult to achieve it, it is advised not to exceed. It does not matter if the adult stops before the two minutes, he can resume the march before the time runs out.
Time: two minutes, both sexes. A minimum of 64 steps must be taken.
Indication: Demonstrate beforehand what the older adult should do.
Means and instruments: measuring tape, stopwatch, chalk, masking tape or other means of marking on the wall and a chair for the rest of the older adult.
Information processing: only one measurement is made.
Test #6. Put your hands behind your back (left and right).
Objective of the test: to evaluate the active flexibility of the arms.
Theoretical foundation: characterized by gradual extension to the limits of stretching, as well as maintenance of flexibility in the upper extremities in old age for greater reach, grip and manipulation of objects.
Procedure
Position: standing in a comfortable position.
Task: raise the predominant arm above the head and flex it while the opposite arm flexes behind the back. Try to touch the middle fingertips of both hands, hold your breath. Do it with both arms.
Indication: perform previous demonstration and give the order to start. If there is pain, stop.
Measure from the center of the palm to the tip of the middle finger, keep the tape straight:
Test #7. Walk six minutes
Objective of the test: to assess aerobic endurance.
Theoretical foundation: aerobic capacity that expresses the possibility of using the aerobic energy mechanism as a fundamental way to obtain energy. Functional physical capacity that allows the state of physical and mental health, active commitment to life in these ages and maintain its functionality, to expand healthy life expectancy, productivity and quality of life in old age.
Procedure
Position: stood.
Task: do the course without exaggerating their physical possibilities, if they get tired must stop and then resume.
Conformation of the area: rectangular area of 46 meters (23 by 2). Within the itinerary marked with cones, every five meters is marked with adhesive tape, mark the number of meters.
Time: six minutes.
Indication: make previous demonstration and give the order to start.
Stimulate the participant and warn him when there are only two minutes left. Participants should perform a relaxation exercise at the end of the test.
Means and instruments: stopwatch, adhesive tape, cones, knobs, chalk, flags or other objects to delimit the terrain and distances.
Protocol: only one route.
Important elements for the implementation of the battery of tests: Every process has several stages, each one constituting a process in itself; they are diagnosis, planning, implementation and evaluation. Each one has a group of specific actions, which allow in the evaluation stage, from their results, the restructuring of the process.
Diagnosis: in this stage, the starting elements for the evaluation are defined. The individual characteristics of each older adult are taken into account for the projection of the evaluation, their age, the age group to which they belong and their sex. The results of this diagnosis are those that allow the individual proposal for each older adult to be kept up to date, to elaborate a proposal for the group in general, and to form working groups.
Planning: this moment corresponds to the stratification of the CNTDs in the target population and in the evaluation standards for each of the age groups according to sex and test requirements, as well as taking into account the inclusion and exclusion criteria, which must be defined precisely beforehand.
Implementation: this is the period that corresponds to the organization of the fieldwork: the space where the tests will be carried out is organized, with the necessary implements in each one; the teachers are distributed according to the task that has been assigned to them, who must know previously the required indications for its realization:
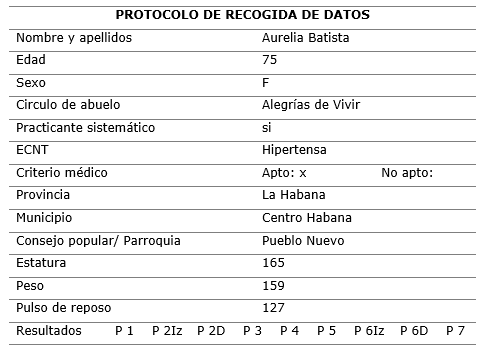
The teacher in charge of the concentration area will receive the participants and will inform them how the measurements will be made. The personal data are then recorded in a spreadsheet and given to the practitioner, who is then transferred successively to the different areas where each test is applied, reflecting the result of each measurement in the spreadsheet.
Subsequently, at the final control table the forms are collected grouped by age groups, sexes and diseases: obese, diabetic, asthmatic, hypertensive and disease-free, for further processing.
Chart 1. - Data collection sheet
Methodological guidelines
In order to guarantee the quality of the evaluators' work with respect to the application of the methodology of each test, as a condition of standardization, it was established that all the exercises selected would be the same and with the same requirements for each and every one of the systematic practitioners of 60 years or more.
RESULTS AND DISCUSSION
Tests to assess physical fitness in older adults who were systematic practitioners in Cuba were represented by 22533. Of these, 14204 females, diversified between those with no base CNTDs and those with some disease, distributed as follows: older adults without base CNTDs 2175, obese 2178, hypertensive 4915, diabetic 4142, and, finally, asthmatics with 794 older adults.
In the male sex 8331 participated, distributed as follows: with CNTDs 1368: obese 1318, hypertensive 2813, diabetic 2402 and with asthma 428.
Test #1. Sitting and rising from a chair in 30s (female)
With the test of sitting and standing in the 30s in the female sex, the best results were concentrated in the group of people who do not present basic CNTD, with a maximum of 19 repetitions and a minimum of 15; in obese and hypertensive, respectively, it was 18 and 14 times.
The group of diabetics presented the lowest repetition values in all age groups in the four percentiles, ranging from 14 to 12, which allows us to affirm that the physical condition that alludes to resistance, to strength, is very disadvantaged in relation to the rest of the diseases.
Test #1. Sitting and standing up from a chair in 30s (male)
The test of sitting and rising in the 30s in the male sex presented, as did the females, the best results in the group that does not present base CNTDS. Repetitions ranged from a maximum of 19 to a minimum of 15; hypertensives and asthmatics in decreasing order: between 19 and 13, and between 18 and 13, respectively.
Test #2. Left forearm flexion and extension with weight in 30s (female)
In the test of endurance to force in the upper extremities in the right forearm, in the female sex, the best results, in the four percentiles, are ratified in the group of people who did not present these diseases and that was represented by the values between 19 and 14, the obese 18 and 15, the hypertensive 17 and 14, diabetics 15 to 12 and finally, the asthmatic represented the maximum in 16 and the minimum in 13.
Test #2. Left forearm flexion and extension with weight in 30s (male)
Left forearm flexion test in 30s in the male sex. The best results, in the four percentiles, are ratified in the group that did not present CNTDS of base, with a maximum of 21 and a minimum of 13. Next, were the obese and hypertensive group, in which it manifests itself in a similar way, which represents 20% of the sample. The strength fluctuated between 19 and 15, the remaining two, the 80th percentile, remained between 17 at most and 14 at least.
Test #2. Right forearm flexion and extension in 30s (female)
The test of right forearm flexion in 30s in the female sex was carried out with the purpose of considering the counter-lateral behavior of the capacity in the opposite limb and in the same variable; the best values are presented in the right limb what can be associated to its condition of dominant limb in the group that does not present CNTDS of base; its ranks oscillated between 20 and 14. The result in the obese showed values between 18 and 15 and the diabetics presented the most depressed values, between 16 and 12, that can be explained given the characteristics of the disease. Finally, asthmatic women presented values between 17 and 14.
Test #2. Right forearm flexion and extension with weight in 30s (male)
The right arm flexion test in the 30s in the male sex showed the best results in the group that does not present base disease, in each of the percentiles analyzed: in the 80th percentile was between 22 and 14 and the 20th percentile, which is the minimum, ranged from a maximum of nine to a minimum of five.
Older male adults, with hypertension as the underlying disease, were the other group with the best behavior: their ranks in the 80th percentile ranged between 20 and 15. Asthmatic adults had values between 18 and 14 and diabetics, the lowest: 17 and 9.
Test #3. Stand up, walk 2.44m and sit down again (female)
The test to stand up, to walk 2,44 m. and to sit again, of the feminine sex, allowed to evaluate the coordinating capacity and its relation with the dynamic balance; the results, were shown of homogeneous way in the group that does not present CNTDS of base in all the percentiles, what evidences that this group of people preserve a better dynamic balance that the rest of the groups, they made it in a minimum of four minutes and a maximum of six. The most unfavorable results can be seen in the obese group, with a minimum of four minutes and a maximum of eight, referred in both cases to the 80th percentile.
Test #3. Stand up, walk 2, 44 m and sit down again (male)
Test stand up walk 2.4 m. 4 m. and sit down again, in the male sex. Here, the results were shown in an equivalent way in the groups made up of people who did not present basic diseases in diabetics and hypertensive women in the 80th percentile. The minimum varied by five and the maximum by six respectively.
It should be noted that the results of the groups, in the different percentiles, are manifested in a different way, because in relation to (MB equivalent to the 80th percentile), the same groups mentioned are maintained with the best values.
Test #4. Bending of the trunk to the front (female)
The flexion of the trunk in the female sex showed the results of the capacity of active flexibility, it is emphasized that the condition of the capacity was taken into account, therefore, the more amplitude shows the adult, having as reference the value zero, the better the results will be; in such sense, the negative values express an evident deficiency in the capacity.
Those declared to have no baseline CNTDS showed the best values at all percentiles; it is understandable that the most deficient values are so far from zero precisely because of the characteristics of capacity at these ages and the loss of capacity, which is intimately related to the loss of range of motion and joint mobility.
Test #4. Bending of the trunk to the front (male)
Bending test of the trunk, in the male sex, it is indicated that the 80th percentile (MB) presented values that were manifested in more than 1 cm. uniformly in all the groups analyzed; on the other hand, the 50th percentile (B) did not vary its central value in relation to the female sex, ratifying this data, the result is (0) in the male sex. The group with no base disease is confirmed, with the best values in all percentiles.
Test #5. Perform two minutes of walking in place (female)
The two-minute walk test, for women, evaluates the physical capacity of mixed resistance, related to the resistance to strength in the lower extremities; it ratifies the group that does not present basic CNTDS as having the best result for each of the percentiles. When evaluating the rest of the groups by percentiles and the behavior of the generated values, it is expressed that the best results were in the diabetics, which independently of the diagnosed disease a predominant tendency is evident as far as the referred physical condition is concerned. The data show that from the 20th percentile downwards, the best values were concentrated in the asthmatic group. With respect to the last percentile, it should be noted that the group of obese women is ratified with the lowest values, which makes it evident that the capacity, in the lower planes, is substantially disadvantaged to the rest of the diseases.
Test #5. Perform two minutes of walking in place (male)
Test perform two minutes of walking on the male sex, when detailing it, it is highlighted that the values fluctuate between 105 and 18 repetitions as maximum and minimum values that were recorded; it is ratified by people who do not have basic diseases as the best percentile result.
When evaluating the rest of the groups by percentiles and the behavior of the values, it could be observed that the best results (80th percentile, MB) were concentrated in the group of diabetics. The remaining groups behaved irregularly, which is evident in the lowest results in this test, which are shown heterogeneously, because in the 80th percentile (MB), the group of obese stands out with the lowest values. On the other hand, in the 20th percentile (R), asthmatics are located and in the <20 percentile (M), the hypertensive group. It is evident that the capacity of resistance to force, in the lower planes, is mostly affected in the obese and asthmatic ones.
Test #6. To put hands behind back with left arm (female).
Test To put hands behind your back with your left arm for female uniform data were shown in a general way by percentiles, the results reveal that the greater of the values in the flexibility of arms behind the back, in this plane, was of 2 cm., therefore, it is correct to raise in the 80th percentile (MB) that this assumes values of 1 or more (cm.). In females, the lowest results were in obese females, presenting values ranging from -1 to -19, in the percentiles relative to R and M.
Test #6. To put hands behind your back with your left arm (male)
Test to put hands behind back (left) for male, the results reveal that the highest value for arm flexibility behind the back, measured from the right, was 2 cm, showing better results than the left arm at the 80th percentile (MB assessment).
Test #6. To put hands behind your back with right arm (female)
Test Top ut hands bihind back (right) for female al respecto, the greater of the values in the flexibility of arms behind the back, measured from the right was 3 cm. or more, showing better results than the left arm in the 80th percentile (MB).
The group with the most unfavourable results was made up of obese people, whose values were shown between -1 and -19 in the percentiles relative to R and M, concentrating in these values 653 in 30 % and 436 adults.
Test #6. To put hands behind back (right hand) for male
To put hands behind back (right hand) for male, revealed that the highest value in arm flexibility, behind the back, was 3 cm, showing better results than the left arm.
Corresponding to the 50th percentile (B evaluation), these values did not vary in relation to the result of the previous test, i.e., it is located at level zero (0). These results corroborate that the active flexibility of arms behind the back behaves with better values from the right sector, however, when comparing the results with the female sex, low results are evidenced in this group. The behaviour of the results for base disease was demonstrated in depth, as it was found that the most significant results were concentrated in the group that does not have base disease. The group with the most unfavourable results was, once again, that of obese adults, which represents 80% of the sample studied.
Test #7. To walk for six minutes (female)
To walk for six minutes for female implies the evaluation of the physical condition of aerobic endurance that is why it was considered as a determining aspect, which would have better physical condition, the older adult who managed to walk a greater distance in a given time. Correspondingly, the general values recorded ranged between 749 m. and 304 m. Due to the quality of the results in all percentiles, the hypertensive group is located. In general, the least significant results with respect to the group that experienced better physical condition were registered by the group of obese women.
Test #7. To walk for six minutes (male)
To walk for si minutes in the male sex experiences greater aerobic endurance than the female sex, being able to travel more meters in the same space of time. In general, the group of obese was the most irregular in the test analyzed.
The assessment of physical condition in older adults, systematic practitioners, takes into account as essential elements the skills, aptitudes for successful performance in the activities of daily life, the independence of the individual and improvement in the performance of their fuCNTDSions.
The selection of exercises should take into account whether they answer the following questions:
In this sense, the following aspects are considered for its application:
It will include all older adults who perform physical activity in grandparent circles, exclude people under 60 years of age, the instruments to be used are specified in each test and must organize seminars or workshops for overcoming professionals who will apply the tests.
There are seven physical tests. The battery presents an organizational structure that gathers from the name of the test, the objective to evaluate, the theoretical foundation and the procedures of action, from the position to adopt, the task to carry out, the time of accomplishment, the activity, indications for the evaluator and means of use.
The battery of tests is based on the principles of active ageing, the theory of organs and systems; it takes into account aspects from a fuCNTDSional, psychopedagogical, philosophical and social point of view; in addition, the capacities to be evaluated in each of the tests are declared as categories; in this, strength and flexibility are related for both hemicorps, coordination capacity and, from it, dynamic balance and, finally, aerobic resistance. It has a system of evaluation tempered to the conditions to these people.
BIBLIOGRAPHICAL REFERENCES
Beratarrechea, A. et al., (2016). Manual para el Cuidado Integral de Personas Adultas en el Primer Nivel de Atención Control de Enfermedades No Transmisibles. Ministerio de salud. Presidencia de la nación. Ciudad de México. Recuperado de https://www.google.com/search?q=Manual+para+el+Cuidado+Integral+de+Personas+Adultas+en+el+Primer+Nivel+de+Atenci%C3%B3n+Control+de+Enfermedades+No+Transmisibles.&ie=utf -8&oe=utf-8&client=firefox-b-ab#
Cuellar, C. S., González, L. M. B., Pacheco, A. M. S., Tejada, A. M. C., Castillo, L. Y. R., Niño, D. M. V., González, M. E. O. (2016). Cualidades físicas del adulto mayor activo de la ciudad de Tunja. Revista Investigación en Salud Universidad de Boyacá, 3(1), 33-49. Recuperado de https://doi.org/10.24267/23897325.140 ; http://revistasdigitales.uniboyaca.edu.co/index.php/rs/article/view/140
Chan, M. (2015). Informe mundial sobre el envejecimiento y la salud. (OMS) Organización Mundial de la Salud. Directora General. Recuperado de https://apps.who.int/iris/bitstream /handle/10665/186471/WHO_FWC_ALC_15.01_spa.pdf;jsessionid=D9864D20D615C63BA50721B7A8
Escalante, L.C. (2015). Evaluación de la condición física en adultos mayores practicantes sistemáticos. Tesis en opción al Grado Científico de Doctor en Ciencias de la Cultura Física. Universidad de Ciencias de la Cultura Física, Manuel Fajardo. La Habana, Cuba.
Giai, M. (2014). Actividades recreativas en adultos mayores internos en un hogar de ancianos. Revista Cubana de Salud Pública, 41(1). 67-76. Recuperado de http://www.revsaludpublica.sld.cu/index.php/spu/article/view/297
Guerrero-R, N., & Yépez-Ch, M. C. (2015). Factors associated with the vulnerability of the elderly with health disorders. Universidad y Salud, 17(1), 121-131. Recuperado de http://www.scielo.org.co/scielo.php?script=sci_abstract&pid=S0124-71072015000100011&lng=en&nrm=iso&tlng=es
Gutiérrez, L.R y Kershenobich, D.S. (2015). Envejecimiento y salud: una propuesta para un plan de acción. Instituto nacional de geriatría. México: UNAM, Coordinación de la Investigación Científica: Dirección General de Publicaciones y Fomento Editorial; Academia Nacional de Medicina de México: Academia Mexicana de Cirugía: Instituto Nacional de Geriatría. 352 págs. Recuperado de http://www.geriatria.salud.gob.mx/descargas/publicaciones /Envejecimiento_y_salud_3a_edicion.pdf.
López, F. (2018). Los derechos humanos de las personas mayores. Cuarta reimpresión. Comisión Nacional de los Derechos Humanos Periférico Sur 3469. Recuperado de http://www.cndh.org.mx/sites/all/doc/cartillas/2015-2016/27-DH-Adultos-Mayores.pdf
Loredo-Figueroa, M. T., Gallegos-Torres, R. M., Xeque-Morales, A. S., Palomé-Vega, G., & Juárez-Lira, A. (2016). Nivel de dependencia, autocuidado y calidad de vida del adulto mayor. Enfermería Universitaria, 13(3), 159-165. Recuperado de https://doi.org/10.1016/j.reu.2016.05.002
Martínez Pérez, T., González Aragón, C., Castellón León, G., & González Aguiar, B. (2018). El envejecimiento, la vejez y la calidad de vida: ¿éxito o dificultad? Revista Finlay, 8(1), 59-65. Recuperado de http://scielo.sld.cu/scielo.php?script=sci_abstract&pid=S2221-24342018000100007&lng=es&nrm=iso&tlng=es
Chacón-Serna, M. J., Quino-Ávila, A. C., & Vallejo-Castillo, L. F. (2017). Capacidad funcional del anciano relacionada con la actividad física. Revista Investigación en Salud Universidad de Boyacá, 4(1), 86-103. Recuperado de https://doi.org/10.24267/23897325.199; https://revistasdigitales.uniboyaca.edu.co/index.php/rs/article/view/199/235
Olivares, D. Y. R., Martínez, L. R., Oquendo, L. de la C. B., & Crespo, F. V. G. (2015). Calidad de vida en el adulto mayor. Varona (digtal). Recuperado de http://revistas.ucpejv.edu.cu/index.php/rVar/article/view/267
Varela-Pinedo, L., Chávez-Jimeno, H., Tello-Rodríguez, T., Ortiz-Saavedra, P., Gálvez-Cano, M., Casas-Vasquez, P., … Ciudad-Fernandez, L. (2015). Perfil clínico, funcional y sociofamiliar del adulto mayor de la comunidad en un distrito de Lima, Perú. Revista Peruana de Medicina Experimental y Salud Publica, 32(4), 709-716. Recuperado de http://www.scielo.org.pe/scielo.php?script=sci_abstract&pid=S1726-46342015000400012&lng=es&nrm=iso&tlng=es
Pinedo, V., & F, L. (2016). Salud y calidad de vida en el adulto mayor. Revista Peruana de Medicina Experimental y Salud Publica, 33(2), 199-201.Recuperado de https://doi.org/10.17843/rpmesp.2016.332.2196
Santillán, M. de L. V., Arana-Gómez, B., García-Hernández, M. de L., Ruelas-González, M. G., Melguizo-Herrera, E., & Ruiz-Martínez, A. O. (2017). Significado de salud: La vivencia del adulto mayor. Aquichan, 17(2), 171-182. Recuperado de https://aquichan.unisabana.edu.co/index.php/aquichan/article/view/6730
![]()
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International license.
Copyright (c) 2019 Leidys Escalante Candeaux